Osteosynthesis of Chronically Displaced Nonunion of Olecranon Fracture Without Bone Grafting
Keiko Amano, MD¹; Mohammed S. Abdullah, BS²; Jeremy S. Somerson, MD¹
¹Department of Orthopedic Surgery & Rehabilitation, University of Texas Medical Branch; Galveston, TX, USA²School of Medicine, University of Texas Medical Branch; Galveston, TX, USA
Corresponding Author:Jeremy S. Somerson, MD, Department of Orthopedic Surgery & Rehabilitation, University of Texas Medical Branch, 301 University Blvd., Galveston, TX 77555, USA; esomers@utmb.edu
DOI: 10.18600/toj.070102
INTRODUCTION
Olecranon fractures are common fractures of the upper extremity which are usually addressed surgically [1]. Nonsurgical treatment with brief immobilization is reserved for older patients with low-demand activity levels, who may also have a higher risk of surgical complications [2,3]. Surgical treatment has a high rate of successful outcomes, with low rates of stiffness and nonunion [1,4]. Because most of these fractures are surgically managed, there is a paucity of literature and guidelines for treatment of chronic nonunions. Reports of nonunions treated surgically are limited. Published reports are usually nonunions that were found after initial surgical treatment [5]. Many have utilized cortical bone graft, usually iliac crest autograft [5-7]. We report a case of chronically displaced nonunion of an olecranon fracture that was initially treated nonoperatively. The patient was treated with osteosynthesis without bone grafting 2 years after his initial injury.
CASE PRESENTATION
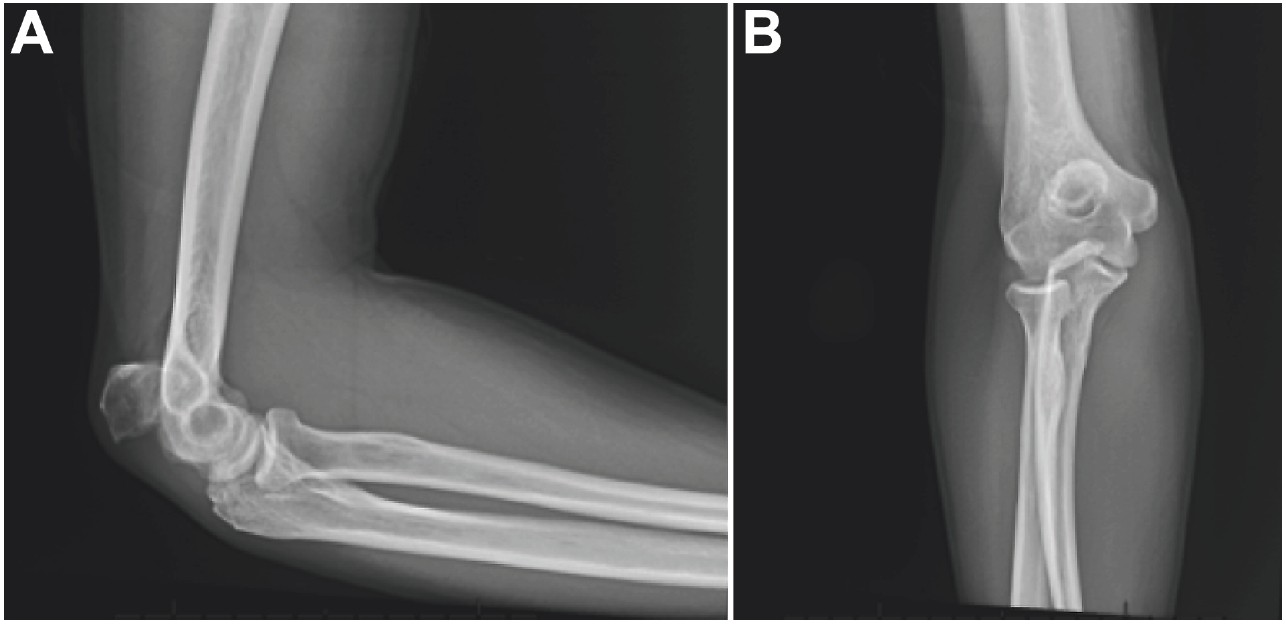
A healthy, 35-year-old male with past history of hypertension presented to our clinic with weakness of right arm after sustaining an olecranon fracture 2 years prior. He stated that at the time of the fracture, he was told he did not need surgery; however, he never regained strength in the affected arm. He also complained of numbness in his small finger at night. He had mild-moderate pain, with a preoperative visual analog score (VAS) of 4. On examination, he had no tenderness to palpation, but a palpable olecranon piece was mobile on physical exam and able to be advanced distally. He had full active range of motion of his elbow, but his elbow extension strength was 2 out of 5. His sensation was decreased in the small finger. His radiographs at the time of presentation to our clinic demonstrate an approximately 27-mm gap between the fragment and the ulna, with atrophic edges (Figure 1).
Examination and radiographs revealed no other injuries. Given the patient’s young age and high activity level, we recommended surgical fixation of his nonunion. We discussed the possibility of losing terminal flexion after surgery due to the chronicity of injury and possible contracture of the triceps. The patient opted for open reduction and internal fixation of the olecranon with ulnar nerve decompression with possible transposition, and possible iliac crest autograft.
TREATMENT
The patient underwent surgery approximately 3 weeks from the date of his presentation. He was placed in supine position, and a standard posterior approach to the proximal ulna was used. The fracture edges were identified and debrided. The debridement revealed healthy bleeding cancellous bone edges, and the edges were able to be positioned in direct apposition with compression. Therefore, we elected not to use autograft. The ulnar nerve was then decompressed through a separate window in situ. The nerve showed no subluxation with flexion and extension of the elbow; thus, we opted not to perform a transposition. The fracture was reduced and clamped and a posterior olecranon plate was selected (Figure 2). The plate was first secured onto bone by placing a screw in the distal oblong screw hole, allowing the plate to be on the bone but still able to slide. Then a longitudinal metaphyseal screw was placed through the proximal plate through the fracture, compressing the plate onto the bone allowing compression of the fracture site. The distal screw was secured, and additional distal and proximal screws were placed for plate fixation. The reduction stayed stable throughout the range of motion.
TREATMENT
The patient underwent surgery approximately 3 weeks from the date of his presentation. He was placed in supine position, and a standard posterior approach to the proximal ulna was used. The fracture edges were identified and debrided. The debridement revealed healthy bleeding cancellous bone edges, and the edges were able to be positioned in direct apposition with compression. Therefore, we elected not to use autograft. The ulnar nerve was then decompressed through a separate window in situ. The nerve showed no subluxation with flexion and extension of the elbow; thus, we opted not to perform a transposition. The fracture was reduced and clamped and a posterior olecranon plate was selected (Figure 2). The plate was first secured onto bone by placing a screw in the distal oblong screw hole, allowing the plate to be on the bone but still able to slide. Then a longitudinal metaphyseal screw was placed through the proximal plate through the fracture, compressing the plate onto the bone allowing compression of the fracture site. The distal screw was secured, and additional distal and proximal screws were placed for plate fixation. The reduction stayed stable throughout the range of motion.
.jpg)
OUTCOME AND FOLLOWUP
After surgery, the patient followed up at 3 weeks, 10 weeks, 16 weeks, 7 months, and 18 months. Postoperatively, he no longer complained of ulnar nerve symptoms. He started range of motion exercises at 3 weeks, as he noted continued stiffness of the elbow. At 10 weeks, he was allowed to bear weight as tolerated for daily activities, but was instructed to avoid heavy lifting until complete healing and complete disappearance of the fracture line could be seen on radiographs. We did not specify a weight, but asked that patients refrain from lifting outside of daily living [8].Of note, at his 18-month visit, the patient had developed olecranon bursitis. The fracture appeared completely healed on radiograph (Figure 3), and he was cleared for heavy lifting. At this point, he had a range of motion of 0 to 150 degrees, with 80 of both supination and pronation with greater than 4 of 5 strength. Hardware removal for irritation is planned upon resolution of his olecranon bursitis. Figure 4 demonstrates the trend in patient-reported outcomes, demonstrating marked improvement after surgery.
.jpg)
REFERENCES
[1] Baecher N, Edwards S. Olecranon fractures. J Hand Surg Am 2013;38(3):593-604.
[2] Duckworth AD, Bugler KE, Clement ND, et al. Nonoperative management of displaced olecranon fractures in low-demand elderly patients. J Bone Joint Surg Am 2014;96(1):67-72.
[3] Batten TJ, Patel NG, Birdsall P. Olecranon fractures: is nonoperative treatment acceptable in older patients? Curr Orthop Pract 2016;27(1):103-6.
[4] Brolin TJ, Throckmorton T. Olecranon fractures. Hand Clin 2015;31(4):581-90.
[5] Danziger MB, Healy WL. Operative treatment of olecranon nonunion. J Orthop Trauma 1992;6(3):290-3.
[6] Rotini R, Antonioli D, Marinelli A, et al. Surgical treatment of proximal ulna nonunion. Chir Organi Mov 2008;91(2):65-70.
[7] Papagelopoulos PJ, Morrey BF. Treatment of nonunion of olecranon fractures. J Bone Joint Surg Br 1994;76(4):627-35.
[8] Beingessner D, Pollock JW, King GJW. Elbow Fractures and Dislocations. In: Court-Brown CM, Heckman JD, McQueen MM, Ricci WM, Iii PT, editors. Rockwood and Green’s Fractures in Adults. 8th ed. Lippincott Williams & Wilkins; 2015. pp. 1180–227.