Ultrasound Guidance for Palmar and Digital Injections: A Cadaveric Study
Matthew McCarley, MD¹; Waakar Divan, BS¹; Usama Salem, MD²; Daniel Torres, MD³
¹Department of Orthopaedic Surgery & Rehabilitation, University of Texas Medical Branch; Galveston; TX, USA²Departemnt of Radiology, University of Texas Medical Branch; Galveston, TX, USA³Hand & Wrist Surgery, Lehigh Valley Hospital-Muhlenberg; Bethlehem, PA, USA
Corresponding Author:Daniel Torres, MD, Lehigh Valley Hospital-Muhlenberg, 2545 Schoenersville Rd., Bethlehem, PA 18017, USA; e-mail: dantor1983@gmail.com
DOI: 10.18600/toj.060101
INTRODUCTION
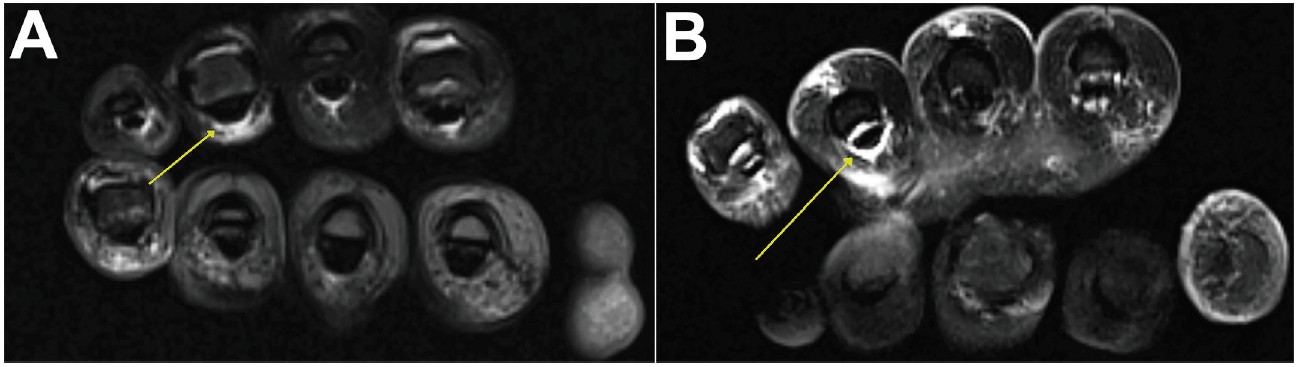
Dupuytren disease (DD) is a fibromatosis of the palmar and digital fascia that forms pathologic nodules and cords and may cause contractures of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints of the fourth and fifth digits. Treatment options for contractures include percutaneous aponeurotomy for milder cases and open fasciectomy for more severe forms [1]. Collagenase injection therapy received FDA approval in 2010 and works via local enzymatic degradation of collagen peptide bonds within the cord structures present directly beneath the skin of the affected palm or digit. The patient typically returns to the office for follow up 1 to 2 days later for cord manipulation [2]. Two multi-center, double-blind, randomized clinical trials evaluating the safety and efficacy of collagenase injection therapy for DD, the CORD I and CORD II trials of 2009 and 2010, enrolled over 1,000 patients with contractures over 20 degrees involving the MCP or PIP joints of the fourth or fifth digits. Collagenase injections were more effective than placebo in correcting contractures to within 5 degrees of full extension. The majority of complications reported were temporary and minor reactions; however, flexor tendon rupture was reported within 1 week in 3 patients (0.3%) [3,4]. After these trials concluded, a few additional cases of flexor tendon rupture have been reported. One involved rupture of both flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons near the small finger MCP joint. In this case, the tendons were repaired primarily [5]. Another involved small-finger FDP rupture near the PIP joint requiring staged reconstruction [6]. Tendon ruptures in these settings are believed to be caused by inadvertent exposure of the underlying tendons to the injected solution, which can render them irreparable due to intrinsic damage from enzymatic degradation. Placing the needle tip deep to the cord structure during the injection places the tendons at risk, although the amount of exposure necessary to cause rupture is unclear. Whether needle penetration of the tendon sheath or tendon proper during the injection predisposes rupture, or whether rupture can occur secondarily via diffusion of the solution despite a well-placed injection, is not known. Key technical aspects of the injection, including avoiding injection near the small finger PIP joint flexion crease and being extremely careful about depth of needle placement in general during the procedure, have been emphasized to minimize this risk. One potential solution is the use of ultrasound guidance to ensure accurate needle placement for the injections. The development of small transducers that provide sufficient resolution of small and superficial structures has made this possible and provides additional diagnostic benefit. Transducers with a frequency of greater than 12MHz in particular have been recommended for hand and wrist applications, and there is some evidence which shows that their use increases accuracy for routine hand and wrist injections [7-9]. For DD, evidence supporting the utility of ultrasound remains limited. The purpose of the present study is to determine whether ultrasound guidance improves injection accuracy in this setting. MATERIALS & METHODS Study Design Palmar and digital injections were performed into the ring and small fingers of 20 matched pair cadaveric hand specimens. All injections were performed by a fellowship-trained hand orthopedic surgeon familiar with collagenase injection technique and the use of ultrasound for hand and wrist diagnostic purposes. Four injections were performed in each hand specimen, for a total of 80 injections performed in the study. For each matched pair of specimens, 1 specimen was randomly selected to receive the 4 injections with ultrasound guidance, and the other was selected to receive the 4 injections without ultrasound (ie, blind technique) as a control. Injection Technique The technique from the Xiaflex® manufacturer’s dosing and administration instructions was followed. 0.25mL of methylene blue dye was injected into the palmar fascia between the distal palmar and palmar-digital creases, and 0.20 mL dye was injected into the digital fascia between the palmar-digital crease and the PIP joint flexion crease. Injections were performed at both the ring and small fingers. A 1-mL syringe with 0.01-mL graduations and a 27-gauge 1/2-inch needle were used for the injections. For the blind injections, palpation of the area preceded needle insertion, and the finger was gently passively manipulated to ensure the needle tip was not in the tendon substance. For the ultrasound-guided injections, an ultrasound machine (GE LOGIQ™ P9) with a 15-MHz hockey stick ultrasound transducer (GE L8-18i-RS) was used, verifying the location of the echogenic needle tip in relation to the flexor tendons and sheath using sagittal and axial probe positioning prior to injection. Data Interpretation Immediately before and after the injections, the specimens were scanned as pairs with magnetic resonance imaging (MRI) (Siemens Verio 3-Tesla model) using axial and sagittal T2-weighted sequences with fat suppression. The MRI scans were interpreted by author US, a musculoskeletal fellowship-trained radiologist. At each injection site, the pre- and post-injection images were compared to determine whether fluid infiltration of the sheath had occurred following injection (Figure 1). The scans were interpreted blinded, without knowledge of which specimens were in each group.
Dupuytren disease (DD) is a fibromatosis of the palmar and digital fascia that forms pathologic nodules and cords and may cause contractures of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints of the fourth and fifth digits. Treatment options for contractures include percutaneous aponeurotomy for milder cases and open fasciectomy for more severe forms [1]. Collagenase injection therapy received FDA approval in 2010 and works via local enzymatic degradation of collagen peptide bonds within the cord structures present directly beneath the skin of the affected palm or digit. The patient typically returns to the office for follow up 1 to 2 days later for cord manipulation [2]. Two multi-center, double-blind, randomized clinical trials evaluating the safety and efficacy of collagenase injection therapy for DD, the CORD I and CORD II trials of 2009 and 2010, enrolled over 1,000 patients with contractures over 20 degrees involving the MCP or PIP joints of the fourth or fifth digits. Collagenase injections were more effective than placebo in correcting contractures to within 5 degrees of full extension. The majority of complications reported were temporary and minor reactions; however, flexor tendon rupture was reported within 1 week in 3 patients (0.3%) [3,4]. After these trials concluded, a few additional cases of flexor tendon rupture have been reported. One involved rupture of both flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons near the small finger MCP joint. In this case, the tendons were repaired primarily [5]. Another involved small-finger FDP rupture near the PIP joint requiring staged reconstruction [6]. Tendon ruptures in these settings are believed to be caused by inadvertent exposure of the underlying tendons to the injected solution, which can render them irreparable due to intrinsic damage from enzymatic degradation. Placing the needle tip deep to the cord structure during the injection places the tendons at risk, although the amount of exposure necessary to cause rupture is unclear. Whether needle penetration of the tendon sheath or tendon proper during the injection predisposes rupture, or whether rupture can occur secondarily via diffusion of the solution despite a well-placed injection, is not known. Key technical aspects of the injection, including avoiding injection near the small finger PIP joint flexion crease and being extremely careful about depth of needle placement in general during the procedure, have been emphasized to minimize this risk. One potential solution is the use of ultrasound guidance to ensure accurate needle placement for the injections. The development of small transducers that provide sufficient resolution of small and superficial structures has made this possible and provides additional diagnostic benefit. Transducers with a frequency of greater than 12MHz in particular have been recommended for hand and wrist applications, and there is some evidence which shows that their use increases accuracy for routine hand and wrist injections [7-9]. For DD, evidence supporting the utility of ultrasound remains limited. The purpose of the present study is to determine whether ultrasound guidance improves injection accuracy in this setting. MATERIALS & METHODS Study Design Palmar and digital injections were performed into the ring and small fingers of 20 matched pair cadaveric hand specimens. All injections were performed by a fellowship-trained hand orthopedic surgeon familiar with collagenase injection technique and the use of ultrasound for hand and wrist diagnostic purposes. Four injections were performed in each hand specimen, for a total of 80 injections performed in the study. For each matched pair of specimens, 1 specimen was randomly selected to receive the 4 injections with ultrasound guidance, and the other was selected to receive the 4 injections without ultrasound (ie, blind technique) as a control. Injection Technique The technique from the Xiaflex® manufacturer’s dosing and administration instructions was followed. 0.25mL of methylene blue dye was injected into the palmar fascia between the distal palmar and palmar-digital creases, and 0.20 mL dye was injected into the digital fascia between the palmar-digital crease and the PIP joint flexion crease. Injections were performed at both the ring and small fingers. A 1-mL syringe with 0.01-mL graduations and a 27-gauge 1/2-inch needle were used for the injections. For the blind injections, palpation of the area preceded needle insertion, and the finger was gently passively manipulated to ensure the needle tip was not in the tendon substance. For the ultrasound-guided injections, an ultrasound machine (GE LOGIQ™ P9) with a 15-MHz hockey stick ultrasound transducer (GE L8-18i-RS) was used, verifying the location of the echogenic needle tip in relation to the flexor tendons and sheath using sagittal and axial probe positioning prior to injection. Data Interpretation Immediately before and after the injections, the specimens were scanned as pairs with magnetic resonance imaging (MRI) (Siemens Verio 3-Tesla model) using axial and sagittal T2-weighted sequences with fat suppression. The MRI scans were interpreted by author US, a musculoskeletal fellowship-trained radiologist. At each injection site, the pre- and post-injection images were compared to determine whether fluid infiltration of the sheath had occurred following injection (Figure 1). The scans were interpreted blinded, without knowledge of which specimens were in each group.
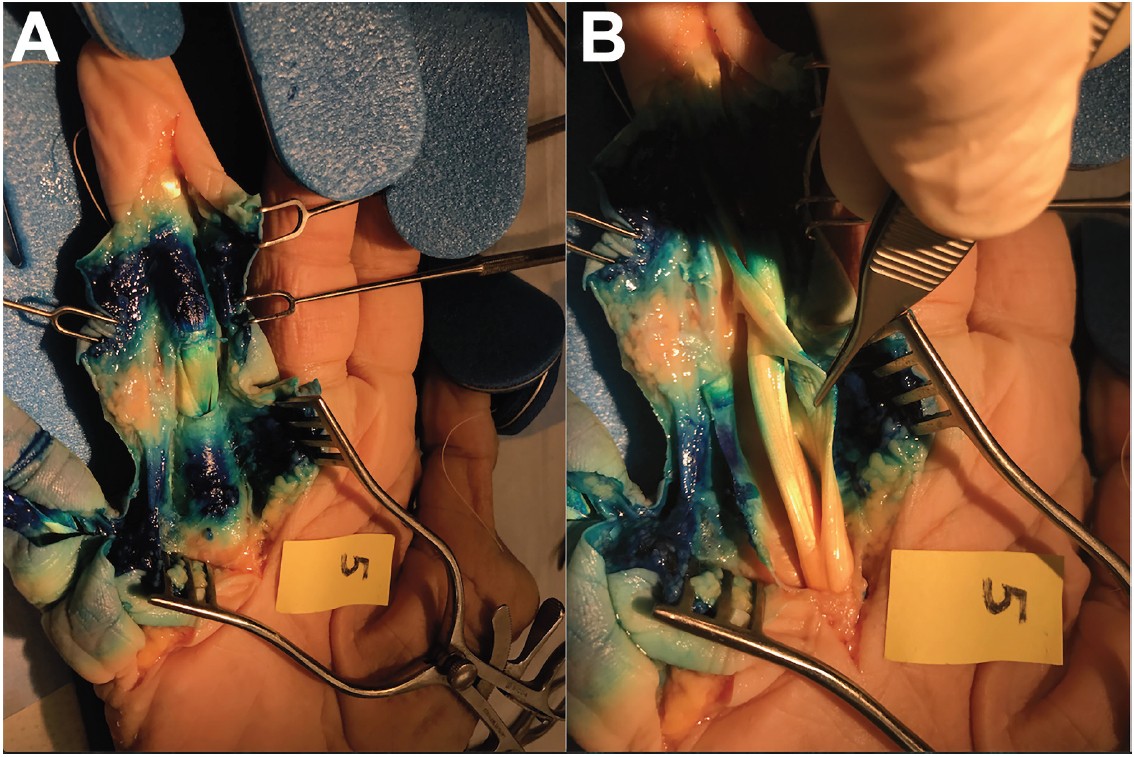
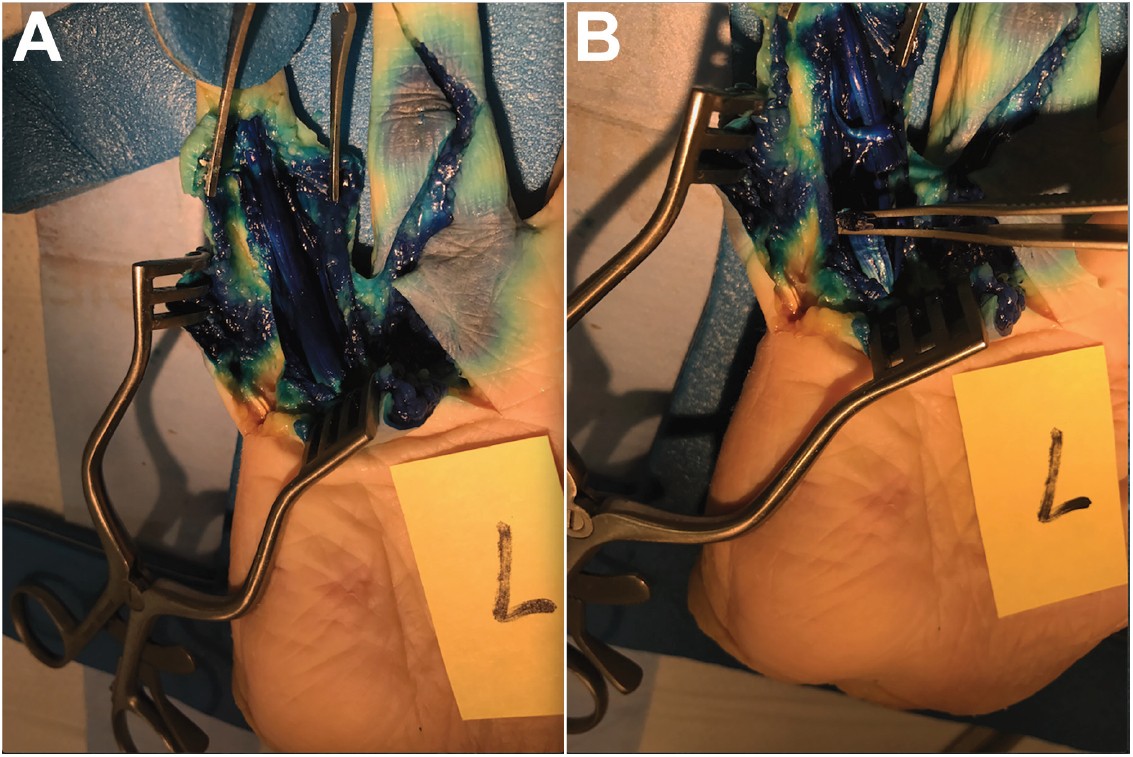
The hand specimens were dissected the day after the injections were performed, using a standard Brunner incision to expose the flexor tendon sheaths in their entirety from the A1 pulley to the fingertip. At each injection site, the extent of tendon exposure to the dye was noted as evidenced by the depth of stain penetration. An injection was deemed to have been placed outside of the sheath if only the superficial side of the tendons was stained, with the undersurface of the tendons remaining white (Figure 2). Conversely, if the entirety of the tendon structure was stained, an injection was considered to have been placed inside the sheath (Figure 3). The dissections were performed blinded, without knowledge of which specimens were in each group.
Using both the MRI and dissection interpretations, an injection was considered to have been erroneously placed if there was evidence of tendon sheath penetration at that particular site in both the MRI and the dissection. In addition to determining an error rate for the injections, the depth from skin surface to flexor tendon was measured using the axial and sagittal MRI sequences at 3 sites in the injection territory at each digit: the distal palmar crease, the palmar-digital crease, and the PIP joint flexion crease.
Statistical Analysis
McNemar’s test was performed to calculate the difference in the injection error rate between the ultrasound-guided injections versus controls. The mean depth of the flexor tendon sheath below skin at the 3 aforementioned sites was also calculated.
RESULTS
MRI Interpretations
In the 40 blind injections fluid was noted completely surrounding the tendons within their sheath (ie, a positive interpretation) at a total of 7 sites (17%): 2 of these were at the ring finger PIP region, 1 was at the small finger MCP region, and 4 were at the small finger PIP region. In the 40 ultrasound-guided injections, 8 (20%) such interpretations were made, 2 at each of the 4 sites studied.
Depth Measurements on MRI
At the small finger, mean distances from skin to flexor tendon sheath were 5.7, 5.6, and 3.1mm at the distal palmar crease, palmar digital crease, and PIP joint flexion crease, respectively. At the ring finger, these mean distances in the same respective order were 5.7, 5.2, and 3.1 mm.Dissection Interpretations
Dye presence was verified in the superficial palmar fascia as 2 discrete injection sites for each digit. In the vast majority of cases, dye was noted to have made contact with the tendon sheath and epitenon layer only, with the majority of the underlying tendon proper being preserved with its characteristic white appearance. Among the 40 injections performed using the blind technique, 4 injections (10%) were noted to have penetrated the sheath as evidenced by complete staining of the entirety of the tendons; 3 of these injections were located at the small finger PIP region and the other was located at the ring finger PIP region. Among the 40 injections performed using ultrasound guidance, 1 injection (2.5%) was noted to have penetrated the sheath at the ring finger PIP region. Of note, none of the injections performed at the MCP region using either technique were noted to have tendon-sheath dye penetration.
Data Interpretation and Analysis
A total of 5 injection sites were noted upon dissection to have dye injected within the sheath. Four of these sites were also noted to have a corresponding positive MRI interpretation, and all of these injections were in the blind injection group. The lone injection site with a positive finding on dissection but a negative finding on MRI was at the ring PIP in 1 specimen in which ultrasound guidance was used. Therefore, we concluded an error rate of 4/40 (10%) for the blind group and 0/40 (0%) for the ultrasound-guided group. These rates were used in the McNemar test calculation. From this test, we found no significant deviation.
DISCUSSION
The role of ultrasound guidance in injections of the hand and wrist has been investigated previously using cadaveric models by Lee et al. [8] and Leversedge et al. [9]. These investigations found that ultrasound-guided injections placed at the A1 pulley (trigger finger) and in the first dorsal compartment (de Quervain’s tenosynovitis) were more accurate than those placed at these locations using traditional blind palpation techniques. Using a similar study design to ours, these authors utilized injected dye to easily identify the location of injected solution during dissection. A notable difference between these studies and ours is our goal of avoiding injection into the tendon sheath or compartment. To mitigate the potential for dispersal of dye during dissection, which could make interpretation difficult, we elected to perform non-invasive interpretation prior to performing the dissections to provide an additional means of interpretation of accuracy.
Although ultrasound guidance has been previously established as an aid for injection accuracy, its role in clinical practice for hand and wrist applications continues to be limited. Surgeons unfamiliar with the technique and who wish to avoid the additional time and effort involved with using an ultrasound machine to perform these injections are hesitant to adopt the technique. Furthermore, our experience with the use of ultrasound to conduct this experiment was that it was cumbersome and, at times, a challenge because of the small working area involved in these injections. Instructional courses offering hands-on demonstrations of the use of ultrasound for common in-office procedures are increasingly available and can allow one to become more familiar and comfortable with this technology.
Another possible explanation for the slow adoption of ultrasound is the mixed results shown in clinical comparative studies with regard to outcomes regarding the use of ultrasound guidance for hand and wrist injections [10-12]. Cecen et al, in a randomized clinical trial comparing ultrasound-guided trigger finger injections to a blind technique, showed no differences in outcomes with regard to symptom resolution between the 2 groups [10]. McDermott et al. performed de Quervain’s injections using ultrasound guidance and found a slightly higher rate of success with their technique compared to standard reported success rates in the literature [11]. Kume et al, in their randomized clinical trial, found that de Quervain’s injections with a separate subcompartment injected using ultrasound guidance had better results compared to those performed blind [12]. There is still insufficient evidence, therefore, to recommend for or against the use of ultrasound guidance for hand and wrist applications on the basis of clinical results.
In the setting of DD, ultrasound imaging has been shown to be an accurate means of identification of nodules and cords as well as their relationship to adjacent tendons and neurovascular bundles as confirmed by follow-up surgical inspection, making it a valuable preoperative imaging modality [13,14]. Leclere et al. provide a case series of 33 patients in which ultrasound guidance was used for collagenase injections for DD. In their study, there were no flexor tendon ruptures, and all patients reported satisfactory results at last follow-up [15]. Therefore, although this study shows that the use of ultrasound in a clinical setting is feasible for these injections, it does not address whether ultrasound guidance improves their accuracy.
There are a few notable limitations to the current study. Normal cadaver hand specimens were utilized for the experiment, as we were unable to obtain specimens specifically affected with DD. This limitation has several implications. The distribution pattern of the injected solution is different within normal palmar and digital fascia as compared to within a pathologic fibrous cord, which would presumably contain more of the solution and help prevent its diffusion into the underlying tendons. Also, the injection technique is different when a cord is involved, in which case several small aliquots of solution are injected along the length of the cord substance as opposed to injecting the entire volume of solution in a single location, as was done in this study. Additionally, when a contracture is present, applying the ultrasound transducer appropriately to the digit to obtain an adequate image is certainly more difficult compared to imaging a digit in full extension. With regard to MRI interpretations, distinguishing the presence of dye surrounding the tendons within their sheaths from normal tenosynovial fluid was notably difficult given the preserved state of the cadaveric specimens. Using gadolinium in the injection solution may have made this distinction more clear. To minimize this limitation, as noted previously, we only considered an injection error to have been present at any given site if its appearance on MRI was also corroborated with the findings determined at the time of dissection.
Although our error rates may suggest otherwise, we conclude that ultrasound guidance adds time to the procedure and does not significantly improve injection accuracy for palmar and digital injections performed in this manner for DD. It remains unclear to what extent exposure of the underlying tendons to collagenase actually results in rupture, specifically whether tendon sheath infiltration during injection—the primary endpoint we evaluated in this study—is necessary to predispose rupture. A randomized clinical trial evaluating the clinical outcomes of blind versus ultrasound-guided collagenase for DD, specifically with regard to tendon rupture complications, is therefore needed to really understand whether the use of ultrasound guidance is warranted in this setting.
REFERENCES
[1] Black EM, Blazar PE. Dupuytren disease: an evolving understanding of an age-old dis-ease. J Am Acad Orthop Surg 2011; 19(12):746-57.
[2] Xiaflex® Drug Label. Auxilium Pharmaceuticals, Inc. http://www.endo.com/File%20Library/Products/Prescribing%20Information Xiaflex_prescribing_information.html. Accessed 23 Nov 2019.
[3] Hurst LC, Badalamente MA, Hentz VR, Hotchkiss RN, Kaplan FTD, Meals RA, Smith TM, Rodzvilla J, CORD I Study Group. Injectable collagenase clostridium histolyticum for Dupuytren’s contracture. N Engl J Med 2009; 361:968-79.
[4] Gilpin D, Coleman S, Hall S, Houston A, Karrasch J, Jones N. Injectable collagenase clostridium histolyticum: a new nonsurgical treatment for Dupuytren’s disease. J Hand Surg Am 2010; 35(12):2027-38.
[5] Povlsen B, Singh S. Acute double flexor tendon ruptures following injection of colla-genase clostridium histolyticum (xiapex) for Dupuytren’s contracture. BMJ Case Rep 2014.
[6] Zhang AY, Curtin CM, Hentz VR. Flexor tendon rupture after collagenase injection for Dupuytren contracture: case report. J Hand Surg Am 2011; 36(8):1323-5.
[7] Starr HM, Sedgley MD, Means KR, Murphy MS. Ultrasonography for hand and wrist conditions. J Am Acad Orthop Surg 2016; 24:544-554.
[8] Lee DH, Han SB, Park JW, Lee SH, Kim KW, Jeong WK. Sonographically guided tendon sheath injections are more accurate than blind injections: implications for trigger finger treatment. J Ultrasound Med 2011; 30(2):197-203.
[9] Leversedge FJ, Cotterell IH, Nickel BT, Crosmer M, Richard M, Angermeier E. Ultrasonography-guided de Quervain injection: accuracy and anatomic considerations in a cadaver model. J Am Acad Orthop Surg 2016; 24(6):399-404.
[10] Cecen GS, Gulabi D, Saglam F, Tanju NU, Bekler HI. Corticosteroid injection for trigger finger: blinded or ultrasound-guided injection? Arch Orthop Trauma Surg 2015; 135(1):125-131.
[11] McDermott JD, et al. Ultrasound-guided injections for de Quervain’s tenosynovitis. Clin Orthop Relat Res 2012; 470(7):1925-31.
[12] Kume K, Amano K, Yamada S, Amano K, Kuwaba N, Ohta H. In de Quervain’s with a separate EPB compartment, ultrasound-guided steroid injection is more effective than a clinical injection technique: a prospective open-label study. J Hand Surg Eur Vol 2012; 37(6):523-7.
[13] Creteur V, Madani A, Gosset N. Ultrasound imaging of Dupuytren’s contracture [French]. J Radiol 2010; 91(6):687-91.
[14] Uehara K, Miura T, Morizaki Y, Miyamoto H, Ohe T, Tanaka S. Ultrasonographic evaluation of displaced neurovascular bundle in Dupuytren disease. J Hand Surg Am 2013; 38(1):23-8.
[15] Leclere FM, Mathys L, Vögelin E. Collagenase injection in Dupuytren’s disease, evaluation of the ultra-sound assisted technique. Chir Main 2014; 33(3):196-203.