Current Concepts: Anatomic Double Bundle Posterior Cruciate Ligament Reconstruction
Mark E. Cinque, MS¹ ; Jorge Chahla, MD, PhD¹ ; Robert F. LaPrade, MD, PhD¹·²
¹ The Steadman Clinic; Vail, CO, USA ²Steadman Philippon Research Institute; Vail, CO, USA
Corresponding Author:Robert F. LaPrade, MD,PhD, Steadman Philippon Research Institute, The Steadman Clinic, 181 West Meadow Drive, Suite 400, Vail, CO 81657; drlaprade@sprivail.org
DOI: 10.18600/toj.020202
INTRODUCTION
Posterior cruciate ligament (PCL) research and surgical technique development has exponentially evolved during the last years, due to the better understanding of the anatomy, biomechanics and improved surgical tools. Early studies reported good outcomes following nonoperative treatment of PCL injuries [1,2]. However, as research and understanding on these injuries have progressed, nonoperative management results have trended towards poor patient outcomes and early osteoarthritis following severe isolated or combined PCL injuries [3-5].
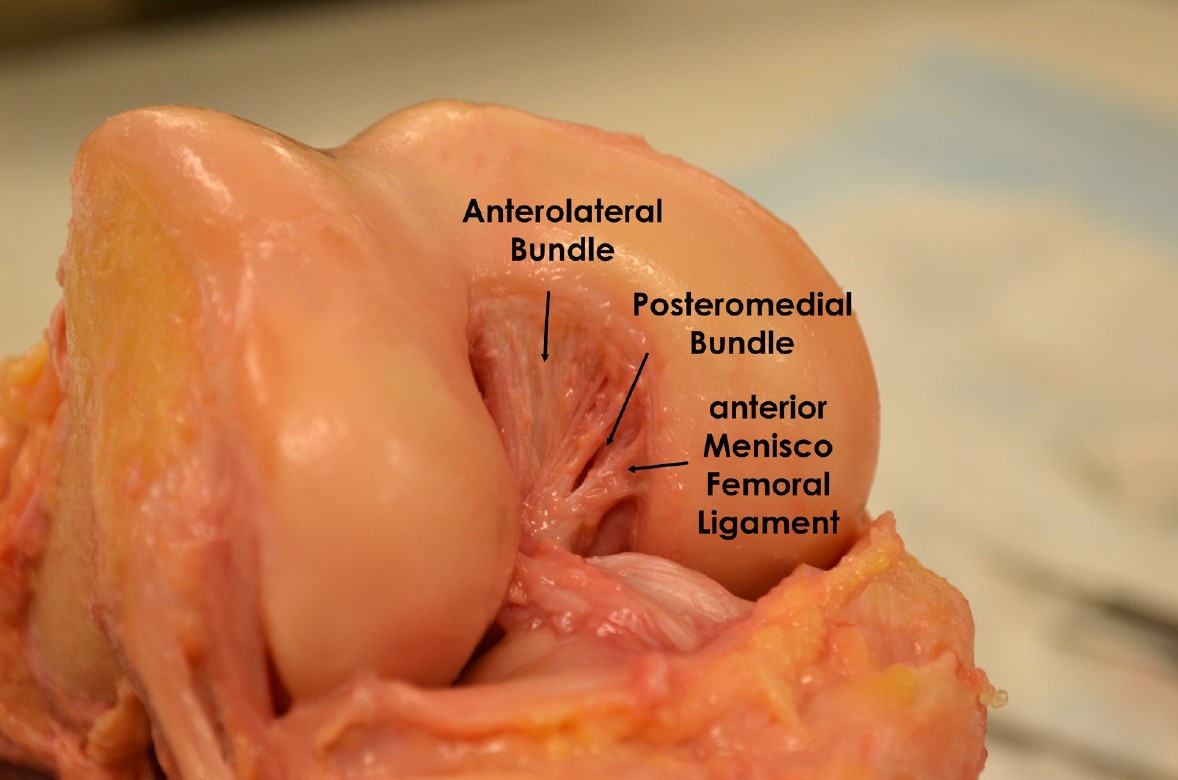
The PCL is an extrasynovial, extra-articular structure that provides resistance to posterior tibial translation. The PCL also acts as a secondary restraint to internal rotation between 90 and 120 degrees of flexion [6]. The PCL is made up of two bundles that act synergistically: the anterolateral bundle (ALB) and the posteromedial bundle (PMB). However, recent biomechanical and anatomic studies have shown that both bundles act in conjunction in the anteroposterior and rotational axes [7,8 ].
PCL injuries often occur in the setting of multiple ligament injury rather than in isolation. Moreover, concomitant chondral and meniscal lesions are commonly seen with PCL injuries [9]. Although isolated PCL injuries are rarer, this subset of patients are at a 6-fold increased risk of developing OA [9].
PCL reconstruction (PCLR) has demonstrated more satisfactory stability when compared to nonoperative treatment in a recent systematic review [10]. Single bundle PCL reconstruction (SB-PCLR) was one of the first operative choices for PCLR. Research has allowed for advanced development into improvements in tunnel location, graft fixation angles and fixation type. However, biomechanical and clinical studies have reported residual laxity following a single bundle procedure [11]. More recently, much effort has been aimed at refining the SB-PCLR and comparing its outcomes to the double bundle PCL reconstruction (DB -PCLR). However, these studies have proved challenging because there are significant differences between graft utilization and tension and tunnel positioning between the two techniques.
Historically, PCLR outcomes have yielded less predictable results when compared to the outcomes of the better studied and more frequently performed anterior cruciate ligament reconstruction (ACLR) [12-14]. This discrepancy in outcomes may be due to surgeons not anatomically reconstructing both PCL bundles, resulting in loss of function of one or both of the bundles. The goal of this article was to review principles of PCL anatomy and biomechanics in addition to discussing the diagnosis and treatment options for complicated PCL injuries, with an emphasis on the double bundle PCL reconstruction technique.
Anatomy
Although the PCL lies within the joint capsule of the knee, it is considered to be extraarticular because it is enclosed in its own synovial sheath [13]. The PCL is a 32‒38 mm long extrasynovial structure that originates from the lateral aspect of the medial femoral condyle at the junction of the medial wall and roof of the intercondylar notch. It passes posteriorly and laterally towards a depression on the posterior aspect of the tibia, bordered by a medial and lateral prominence [15,16]. The midsubstance portion of the ligament is most compact with an average diameter of 11 mm and makes up approximately one-third of the diameter of the tibial and femoral origins. The ALB has approximately twice the cross-sectional diameter of the PLB [17,18]. Additionally, there are variable anterior and posterior meniscofemoral ligaments [17,19]. Anatomic studies have demonstrated that one or both meniscofemoral ligaments is present in 95% of cadavers while both ligaments are present in 60% of cadaver specimens [20].
The PCL has multiple functional anatomical regions defined by tensioning patterns. The ALB serves as the primary restraint to posterior tibial translation of the knee and is at greatest tension at 90 degrees of flexion. The PMB resists posterior tibial translation as the knee approaches full extension and has been reported to function as a secondary restraint to rotation [6,21]. The tension patterns of the two bundles act in reciprocal patterns as the knee proceeds through its range of motion with few fibers exhibiting isometric behavior.
Biomechanics
The ALB is the strongest bundle in the PCL. Studies have demonstrated that the mean ultimate load to produce failure is 1,120± 362 N. This force is three times more than the mean ultimate load to failure of the PMB (419±128N) [17]. Studies have reported near anatomic knee kinematics when only the PMB was sectioned, leading many to suggest that the ALB plays a more important role in joint stability, and thus a single-bundle PCL reconstruction should be sufficient [21,22]. Conversely, Kennedy et al. reported similar results but instead of sectioning the PMB, they sectioned the ALB and left the PMB intact. These findings demonstrate that both PCL bundles have a co-dominant and synergistic role in native knee kinematics [23].
The length of the PCL varies through the range of motion of the knee. PCL length increases from 0‒90 and remains mostly constant from 105‒120 degrees. PCL length decreases from 120‒135 degrees [7,24-26]. Further research has shown that the ALB becomes more vertical and longer as the knee progresses into flexion [27]. The PMB follows an opposite pattern: it becomes shorter and more horizontal with progressive flexion. The horizontal orientation of the PMB during flexion provides a restraining force to more effectively resist posterior tibial translation. The ALB further bolsters this resistance of posterior tibial translation by becoming less horizontal during progressive flexion. Taken together, these biomechanical studies have elucidated that the PCL is a nonisometric structure with inequitable tension throughout a full range of knee motion and act in a reciprocal fashion to resist posterior tibial translation. Furthermore, the kinematic relationship between the two bundles has implications for surgical reconstructions when considering graft fixation. Fixation of the graft at less than 90 degrees of flexion, as is commonly done for the PMB, may overconstrain the knee at higher flexion angles following surgery.
The PCL also plays a significant role in rotational stability, primarily at higher flexion angles [23,28]. Furthermore, biomechanical studies have shown significant constraint of the PCL to internal rotation at 90 degrees and beyond [23,28]. Specifically, the PMB is the primary structure maintaining both posterior translation and rotational stability at flexion beyond 90 degrees. This is an important finding when considering SB-PCLR, which fails to reconstitute the PM bundle, causing suboptimal posterior and rotational stability [23,28].
Injury Demographics and Evolution
Isolated PCL injuries often occur following dashboard injury, high impact injuries onto a flexed knee or hyperextension of the knee [29]. Recent studies have reported that the incidence of isolated PCL tears was 2 per 100,000 in the general population, and most often in male subjects [9]. Although seemingly rare, these numbers are likely greater than reported due to surgeons missing PCL tears and patients presenting distant from time of injury. Multiligament injures that include PCL tears are more likely following trauma with rotational or valgus/varus stress [29].
PCL deficiency exposes the knee to abnormal knee kinematics and elevated contact pressures in the medial compartment and the patellofemoral joint. This change in kinematics stresses the posterolateral knee structures, placing them at elevated risk of subsequent injury [30]. This increased risk of injury was recently studied in a series of patients with isolated PCL tears at 12-years follow-up. Patients were found to have a 6.2 times increased risk for OA and 3.2 times increased risk for total knee arthroplasty compared to patients without PCL tears. Moreover, studies have demonstrated degenerative cartilage lesions on the medial femoral condyle in 77.8% and the patellar in 46.7% of PCL deficient patients followed for more than five years after their index injury [3].
Diagnosis
After obtaining a thorough history from the patient regarding injury mechanism, symptom type and activity limitation a physical exam should be performed. There are four cardinal tests that should be performed: the posterior drawer test, posterior sag test, quadriceps activation test, and the supine internal rotation (IR) test. The posterior drawer test is performed with the knee flexed to 90 degrees and is best at identifying PCL insufficiency. With the knee flexed to 90 degrees, the anterior tibial condyles should be anterior to the femoral condyles by approximately 10 mm in a PCL-intact knee. A posterior drawer of greater than or equal to 5 mm of increased posterior tibial translation is representative of a grade I PCL tear. Grade II PCL tears are defined by 5‒10 mm of increased posterior tibial translation on posterior drawer exam while greater than 10 mm of increased posterior translation defines a grade III PCL tear. The posterior sag exam is performed at 90 degrees of hip and knee flexion, while applying a posterior force on the tibia. A difference in posterior displacement between the injured and uninjured knees indicates the presence of a PCL injury. The quadriceps activation test can also aid in diagnosing a PCL injury. For this test, the patient is placed in the supine position with the knee is flexed to 90 degrees and the foot resting on the table. In the uninjured knee, quadriceps activation will result in no increase in anterior translation of the tibia. In a PCL-deficient knee, the tibia subluxes posteriorly and quadriceps activation will cause anterior translation of the tibia relative to the femur. If anterior translation is observed, a PCL tear should be suspected. Finally, the supine IR test has been described as an additional way to diagnose PCL injuries [31]. To perform this test, the surgeon assesses tibial internal rotation compared to the uninjured leg at various flexion angles. Recent studies reported a sensitivity of 95.5% and a specificity of 97.1%, in addition to a positive predictive value of 72.4% and negative predictive value of 99.6% for the diagnosis of grade III PCL injuries. Moreover, posterolateral corner injuries have a significant interaction with the supine IR test, increasing its sensitivity and decreasing its specificity.
Imaging
In the acute setting, plain AP and lateral radiographs can aid in diagnosing a PCL bony avulsion. These injuries should be suspected if a patient has posterior instability and has a bony fragment visible on plain radiography. If a bony fragment cannot be visualized but a bony avulsion is suspected, MRI can be performed.
MRI is the most useful means to diagnose a PCL injury acutely [5]. Unfortunately, MRI scans have proven to be less useful in the chronic PCL injury setting. However, other imaging modalities, such as stress radiographs, have emerged as reliable and effective in chronic PCL injuries.
Posterior cruciate ligament (PCL) research and surgical technique development has exponentially evolved during the last years, due to the better understanding of the anatomy, biomechanics and improved surgical tools. Early studies reported good outcomes following nonoperative treatment of PCL injuries [1,2]. However, as research and understanding on these injuries have progressed, nonoperative management results have trended towards poor patient outcomes and early osteoarthritis following severe isolated or combined PCL injuries [3-5].
The PCL is an extrasynovial, extra-articular structure that provides resistance to posterior tibial translation. The PCL also acts as a secondary restraint to internal rotation between 90 and 120 degrees of flexion [6]. The PCL is made up of two bundles that act synergistically: the anterolateral bundle (ALB) and the posteromedial bundle (PMB). However, recent biomechanical and anatomic studies have shown that both bundles act in conjunction in the anteroposterior and rotational axes [7,8 ].
PCL injuries often occur in the setting of multiple ligament injury rather than in isolation. Moreover, concomitant chondral and meniscal lesions are commonly seen with PCL injuries [9]. Although isolated PCL injuries are rarer, this subset of patients are at a 6-fold increased risk of developing OA [9].
PCL reconstruction (PCLR) has demonstrated more satisfactory stability when compared to nonoperative treatment in a recent systematic review [10]. Single bundle PCL reconstruction (SB-PCLR) was one of the first operative choices for PCLR. Research has allowed for advanced development into improvements in tunnel location, graft fixation angles and fixation type. However, biomechanical and clinical studies have reported residual laxity following a single bundle procedure [11]. More recently, much effort has been aimed at refining the SB-PCLR and comparing its outcomes to the double bundle PCL reconstruction (DB -PCLR). However, these studies have proved challenging because there are significant differences between graft utilization and tension and tunnel positioning between the two techniques.
Historically, PCLR outcomes have yielded less predictable results when compared to the outcomes of the better studied and more frequently performed anterior cruciate ligament reconstruction (ACLR) [12-14]. This discrepancy in outcomes may be due to surgeons not anatomically reconstructing both PCL bundles, resulting in loss of function of one or both of the bundles. The goal of this article was to review principles of PCL anatomy and biomechanics in addition to discussing the diagnosis and treatment options for complicated PCL injuries, with an emphasis on the double bundle PCL reconstruction technique.
Anatomy
Although the PCL lies within the joint capsule of the knee, it is considered to be extraarticular because it is enclosed in its own synovial sheath [13]. The PCL is a 32‒38 mm long extrasynovial structure that originates from the lateral aspect of the medial femoral condyle at the junction of the medial wall and roof of the intercondylar notch. It passes posteriorly and laterally towards a depression on the posterior aspect of the tibia, bordered by a medial and lateral prominence [15,16]. The midsubstance portion of the ligament is most compact with an average diameter of 11 mm and makes up approximately one-third of the diameter of the tibial and femoral origins. The ALB has approximately twice the cross-sectional diameter of the PLB [17,18]. Additionally, there are variable anterior and posterior meniscofemoral ligaments [17,19]. Anatomic studies have demonstrated that one or both meniscofemoral ligaments is present in 95% of cadavers while both ligaments are present in 60% of cadaver specimens [20].
The PCL has multiple functional anatomical regions defined by tensioning patterns. The ALB serves as the primary restraint to posterior tibial translation of the knee and is at greatest tension at 90 degrees of flexion. The PMB resists posterior tibial translation as the knee approaches full extension and has been reported to function as a secondary restraint to rotation [6,21]. The tension patterns of the two bundles act in reciprocal patterns as the knee proceeds through its range of motion with few fibers exhibiting isometric behavior.
Biomechanics
The ALB is the strongest bundle in the PCL. Studies have demonstrated that the mean ultimate load to produce failure is 1,120± 362 N. This force is three times more than the mean ultimate load to failure of the PMB (419±128N) [17]. Studies have reported near anatomic knee kinematics when only the PMB was sectioned, leading many to suggest that the ALB plays a more important role in joint stability, and thus a single-bundle PCL reconstruction should be sufficient [21,22]. Conversely, Kennedy et al. reported similar results but instead of sectioning the PMB, they sectioned the ALB and left the PMB intact. These findings demonstrate that both PCL bundles have a co-dominant and synergistic role in native knee kinematics [23].
The length of the PCL varies through the range of motion of the knee. PCL length increases from 0‒90 and remains mostly constant from 105‒120 degrees. PCL length decreases from 120‒135 degrees [7,24-26]. Further research has shown that the ALB becomes more vertical and longer as the knee progresses into flexion [27]. The PMB follows an opposite pattern: it becomes shorter and more horizontal with progressive flexion. The horizontal orientation of the PMB during flexion provides a restraining force to more effectively resist posterior tibial translation. The ALB further bolsters this resistance of posterior tibial translation by becoming less horizontal during progressive flexion. Taken together, these biomechanical studies have elucidated that the PCL is a nonisometric structure with inequitable tension throughout a full range of knee motion and act in a reciprocal fashion to resist posterior tibial translation. Furthermore, the kinematic relationship between the two bundles has implications for surgical reconstructions when considering graft fixation. Fixation of the graft at less than 90 degrees of flexion, as is commonly done for the PMB, may overconstrain the knee at higher flexion angles following surgery.
The PCL also plays a significant role in rotational stability, primarily at higher flexion angles [23,28]. Furthermore, biomechanical studies have shown significant constraint of the PCL to internal rotation at 90 degrees and beyond [23,28]. Specifically, the PMB is the primary structure maintaining both posterior translation and rotational stability at flexion beyond 90 degrees. This is an important finding when considering SB-PCLR, which fails to reconstitute the PM bundle, causing suboptimal posterior and rotational stability [23,28].
Injury Demographics and Evolution
Isolated PCL injuries often occur following dashboard injury, high impact injuries onto a flexed knee or hyperextension of the knee [29]. Recent studies have reported that the incidence of isolated PCL tears was 2 per 100,000 in the general population, and most often in male subjects [9]. Although seemingly rare, these numbers are likely greater than reported due to surgeons missing PCL tears and patients presenting distant from time of injury. Multiligament injures that include PCL tears are more likely following trauma with rotational or valgus/varus stress [29].
PCL deficiency exposes the knee to abnormal knee kinematics and elevated contact pressures in the medial compartment and the patellofemoral joint. This change in kinematics stresses the posterolateral knee structures, placing them at elevated risk of subsequent injury [30]. This increased risk of injury was recently studied in a series of patients with isolated PCL tears at 12-years follow-up. Patients were found to have a 6.2 times increased risk for OA and 3.2 times increased risk for total knee arthroplasty compared to patients without PCL tears. Moreover, studies have demonstrated degenerative cartilage lesions on the medial femoral condyle in 77.8% and the patellar in 46.7% of PCL deficient patients followed for more than five years after their index injury [3].
Diagnosis
After obtaining a thorough history from the patient regarding injury mechanism, symptom type and activity limitation a physical exam should be performed. There are four cardinal tests that should be performed: the posterior drawer test, posterior sag test, quadriceps activation test, and the supine internal rotation (IR) test. The posterior drawer test is performed with the knee flexed to 90 degrees and is best at identifying PCL insufficiency. With the knee flexed to 90 degrees, the anterior tibial condyles should be anterior to the femoral condyles by approximately 10 mm in a PCL-intact knee. A posterior drawer of greater than or equal to 5 mm of increased posterior tibial translation is representative of a grade I PCL tear. Grade II PCL tears are defined by 5‒10 mm of increased posterior tibial translation on posterior drawer exam while greater than 10 mm of increased posterior translation defines a grade III PCL tear. The posterior sag exam is performed at 90 degrees of hip and knee flexion, while applying a posterior force on the tibia. A difference in posterior displacement between the injured and uninjured knees indicates the presence of a PCL injury. The quadriceps activation test can also aid in diagnosing a PCL injury. For this test, the patient is placed in the supine position with the knee is flexed to 90 degrees and the foot resting on the table. In the uninjured knee, quadriceps activation will result in no increase in anterior translation of the tibia. In a PCL-deficient knee, the tibia subluxes posteriorly and quadriceps activation will cause anterior translation of the tibia relative to the femur. If anterior translation is observed, a PCL tear should be suspected. Finally, the supine IR test has been described as an additional way to diagnose PCL injuries [31]. To perform this test, the surgeon assesses tibial internal rotation compared to the uninjured leg at various flexion angles. Recent studies reported a sensitivity of 95.5% and a specificity of 97.1%, in addition to a positive predictive value of 72.4% and negative predictive value of 99.6% for the diagnosis of grade III PCL injuries. Moreover, posterolateral corner injuries have a significant interaction with the supine IR test, increasing its sensitivity and decreasing its specificity.
Imaging
In the acute setting, plain AP and lateral radiographs can aid in diagnosing a PCL bony avulsion. These injuries should be suspected if a patient has posterior instability and has a bony fragment visible on plain radiography. If a bony fragment cannot be visualized but a bony avulsion is suspected, MRI can be performed.
MRI is the most useful means to diagnose a PCL injury acutely [5]. Unfortunately, MRI scans have proven to be less useful in the chronic PCL injury setting. However, other imaging modalities, such as stress radiographs, have emerged as reliable and effective in chronic PCL injuries.
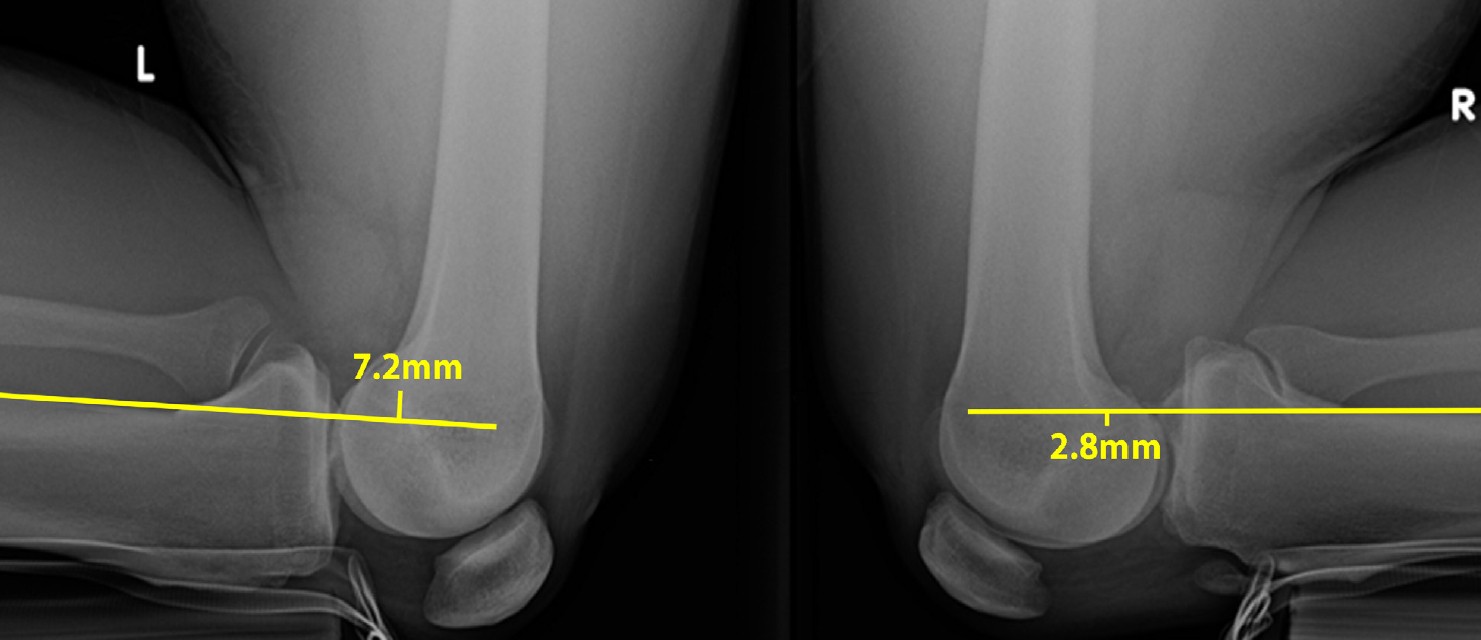
Stress radiographs are essential in evaluating patients with both acute and chronic posterior knee instability. This radiographic modality is a reproducible method to quantify instability. Jackman et al. described kneeling stress radiographs as an ideal method to compare the amount of posterior translation between the injured and uninured knees [32]. From a technical standpoint, a 90 degrees support jig is constructed to ensure comfortable, stable and reproducible positioning of the patient during radiography [32]. Patients are instructed to support their full weight on their tibial tubercles, without placing any weight on their patella to provide consistent posterior force. On the lateral radiograph, a line is drawn along the posterior aspect of the tibia. A perpendicular line is then drawn from the posterior aspect of Blumensaat’s line to the initial line drawn. The distance covered by the perpendicular line represents the amount of posterior tibial translation (Figure 1).
Surgical Techniques and Considerations
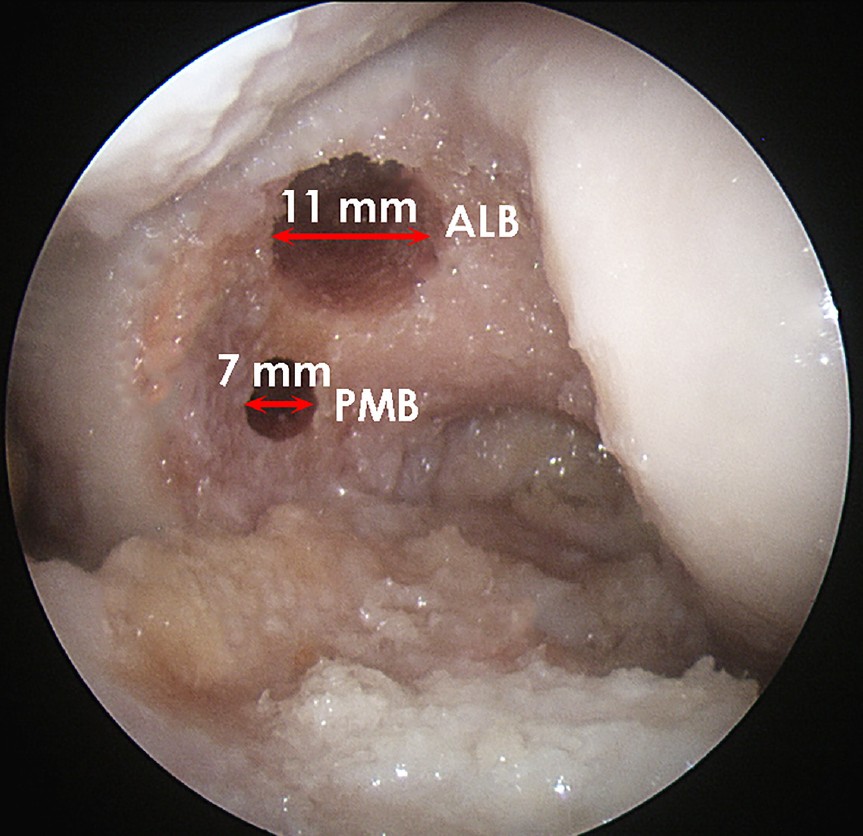
Before the surgical techniques options are weighed, patient specific factors must be considered. The severity of the knee injury (isolated vs. multiligament), grade of PCL injury, acute vs. chronic, clinical presentation (asymptomatic vs. pain/instability) and patient demands or activity level [33]. In general, isolated grade I or II PCL injuries are treated nonoperatively. In order to classify PCL tears as isolated the following conditions must be met: PCL stress radiographs with less than 8 mm differences, less than 5 degrees of rotary laxity at 30 degrees of flexion and no significant varus/valgus instability indicative of mediolateral insufficiency. For isolated PCL tears, the treatment goal is to counteract the posterior laxity of the knee [34]. Dynamic braces now exist that are capable of applying forces to the posterior proximal tibia in a progressive nature with increasing knee flexion angles [35]. Operative intervention is indicated in cases of isolated, symptomatic grade III PCL tears, multiligament injuries requiring reconstruction or when the PCL tear is combined with meniscal body or root tears following an acute injury. Additionally, PCL repair is indicated in cases of PCL bony avulsions, which tend to involve the attachment site of the PCL, and often the meniscal roots, and have emerged as the primary indication for PCL repair. In these cases, surgery should be performed within three weeks from time of injury. Regarding PCL reconstruction, there has been much research and controversy in determining whether the SB-PCLR or DB-PCLR is a superior procedure. Because the PCL has two anatomic bundles that interact kinematically, more attention has been paid recently to the DB-PCLR, as it is thought to provide more reliable resistance to posterior tibial translation and rotation. Recent studies have corroborated this hypothesis in robotic studies by showing that the DB-PCLR are significantly better at restoring knee kinematics as compared to SB-PCLR [28]. Endoscopic double bundle PCL reconstruction is a technically challenging procedure but has demonstrated good outcomes. As previously highlighted, the PCL is composed of two bundles, each with individual and collective roles in knee motion and stability. Because both bundles of the PCL are crucial to prevent posterior tibial translation, surgeons have turned more attention to performing the DB-PCLR, as it represents a more "anatomic" reconstruction than the SB-PCLR [2]. Increased attention has also developed around anatomically reliable landmarks during PCLR. The femoral attachment of the PCL is approximately 32 mm in diameter, with the ALB attaching to the roof and the PMB attaching to the wall of the medial intercondylar notch. The femoral attachment site of the ALB is more proximal and is found at the medial intercondylar ridge while the femoral attachment of the PMB is found at the medial bifurcate ridge [36,37]. The distal margins of the ALB and PMB are 1.5 mm (±0.8) and 5.8 (±1.7) proximal from the notch articular cartilage, respectively [39]. The two bundles join to create a PCL femoral attachment site with a midpoint 7-8 mm proximal to the articular surface. The distance between the ALB and PMB centers are approximately 12.1 mm (±1.3mm) apart [39]. These distances play an important role in surgical planning because recent studies have shown the clock-face method to have poor clinical accuracy and reproducibility [41]. Because of this, Anderson et al. proposed reliable arthroscopic landmarks to guide tunnel placement intraoperatively [39]. The center of the femoral ALB tunnel is found within three important anatomical landmarks: the trochlear point, the medial arch point and the medial bifurcate prominence (Figure 2). These landmarks produce a triangle that around the ALB attachment site. When locating the placement of the PMB, it should be placed halfway from the posterior point and the medial arch point in the femur, distal to the medial intercondylar ridge, approximately 8.6 mm from the distal cartilage margin. With the aforementioned 12.1 mm distance between the two bundles, using an 11-mm ALB and 7-mm PMB tunnels leaves a 2-3 mm bone bridge between tunnels. Recent studies have reported the femoral insertion site to be approximately 128mm, easily large enough to accommodate both tunnels [42].
Before the surgical techniques options are weighed, patient specific factors must be considered. The severity of the knee injury (isolated vs. multiligament), grade of PCL injury, acute vs. chronic, clinical presentation (asymptomatic vs. pain/instability) and patient demands or activity level [33]. In general, isolated grade I or II PCL injuries are treated nonoperatively. In order to classify PCL tears as isolated the following conditions must be met: PCL stress radiographs with less than 8 mm differences, less than 5 degrees of rotary laxity at 30 degrees of flexion and no significant varus/valgus instability indicative of mediolateral insufficiency. For isolated PCL tears, the treatment goal is to counteract the posterior laxity of the knee [34]. Dynamic braces now exist that are capable of applying forces to the posterior proximal tibia in a progressive nature with increasing knee flexion angles [35]. Operative intervention is indicated in cases of isolated, symptomatic grade III PCL tears, multiligament injuries requiring reconstruction or when the PCL tear is combined with meniscal body or root tears following an acute injury. Additionally, PCL repair is indicated in cases of PCL bony avulsions, which tend to involve the attachment site of the PCL, and often the meniscal roots, and have emerged as the primary indication for PCL repair. In these cases, surgery should be performed within three weeks from time of injury. Regarding PCL reconstruction, there has been much research and controversy in determining whether the SB-PCLR or DB-PCLR is a superior procedure. Because the PCL has two anatomic bundles that interact kinematically, more attention has been paid recently to the DB-PCLR, as it is thought to provide more reliable resistance to posterior tibial translation and rotation. Recent studies have corroborated this hypothesis in robotic studies by showing that the DB-PCLR are significantly better at restoring knee kinematics as compared to SB-PCLR [28]. Endoscopic double bundle PCL reconstruction is a technically challenging procedure but has demonstrated good outcomes. As previously highlighted, the PCL is composed of two bundles, each with individual and collective roles in knee motion and stability. Because both bundles of the PCL are crucial to prevent posterior tibial translation, surgeons have turned more attention to performing the DB-PCLR, as it represents a more "anatomic" reconstruction than the SB-PCLR [2]. Increased attention has also developed around anatomically reliable landmarks during PCLR. The femoral attachment of the PCL is approximately 32 mm in diameter, with the ALB attaching to the roof and the PMB attaching to the wall of the medial intercondylar notch. The femoral attachment site of the ALB is more proximal and is found at the medial intercondylar ridge while the femoral attachment of the PMB is found at the medial bifurcate ridge [36,37]. The distal margins of the ALB and PMB are 1.5 mm (±0.8) and 5.8 (±1.7) proximal from the notch articular cartilage, respectively [39]. The two bundles join to create a PCL femoral attachment site with a midpoint 7-8 mm proximal to the articular surface. The distance between the ALB and PMB centers are approximately 12.1 mm (±1.3mm) apart [39]. These distances play an important role in surgical planning because recent studies have shown the clock-face method to have poor clinical accuracy and reproducibility [41]. Because of this, Anderson et al. proposed reliable arthroscopic landmarks to guide tunnel placement intraoperatively [39]. The center of the femoral ALB tunnel is found within three important anatomical landmarks: the trochlear point, the medial arch point and the medial bifurcate prominence (Figure 2). These landmarks produce a triangle that around the ALB attachment site. When locating the placement of the PMB, it should be placed halfway from the posterior point and the medial arch point in the femur, distal to the medial intercondylar ridge, approximately 8.6 mm from the distal cartilage margin. With the aforementioned 12.1 mm distance between the two bundles, using an 11-mm ALB and 7-mm PMB tunnels leaves a 2-3 mm bone bridge between tunnels. Recent studies have reported the femoral insertion site to be approximately 128mm, easily large enough to accommodate both tunnels [42].
The tibial PCL insertion is more compact and thus produces more challenging approach. The tibial PCL insertion site is more compact and converges in a compact fovea on the posterior aspect on the tibia [13,39,40]. Anderson et al. demonstrated a 8.9-mm distance between the bundles, making the drilling of two separate tunnels impractical [42].
However, the shiny white fibers of the posterior horn of the medial meniscus have been shown to be a reliable anterior landmark of the tibial PCL footprint. Additionally, the bony prominence termed the ‘bundle ridge’ reliably defines the posterior margin of the ALB and the anterior margin of the PMB [39]. It is crucial to ensure that the tunnel is not placed posteriorly or inferiorly as these positions will fail to produce an anatomic reconstruction and exposes the popliteal neurovascular structures to injury (Figure 3) [43]. Clinical Outcomes of DB-PCL Reconstructions
Although anatomical and biomechanical studies have been successful in showing decreased posterior tibial translation and increased rotational stability following PCLR, outcomes studies have produced more equivocal results. A recent systematic review compared outcomes of nonoperative management and PCLR in isolated PCL injuries. Conservative management produced a success rate of 33% while surgical intervention resulted in a 90% success rate. Moreover, side to side difference as measured by Telos, ranged from 2.0 to 3.7 in the surgical group and from 3.5 to 5.3 in the nonoperative group. Lastly, and perhaps most importantly, the nonoperative group had more residual anterior-posterior laxity than the surgical group. The combination of these results allowed the study to conclude that surgical intervention produces more satisfactory and consistent stability [10]. Comparing the outcomes of SB-PCLR and DB-PCLR is important to ensure that the previously discussed anatomical superiority of the DB-PCLR indeed produces better biomechanical and clinical outcomes. A recent systematic review concluded that DB-PCLR was significantly superior over SB-PCLR from a biomechanical standpoint [14]. However, no significant difference was found between the two techniques with respect to clinical outcomes at this point in time [14]. Similarly, Harner et al. found the DB-PCLR to be biomechanically superior with regard to posterior tibial translation when they compared SB-PCLR to normal knees and DB-PCLR to normal knees [8]. These studies highlight the superior biomechanics and the lack of robust clinical outcomes following DB-PCLR.
However, the shiny white fibers of the posterior horn of the medial meniscus have been shown to be a reliable anterior landmark of the tibial PCL footprint. Additionally, the bony prominence termed the ‘bundle ridge’ reliably defines the posterior margin of the ALB and the anterior margin of the PMB [39]. It is crucial to ensure that the tunnel is not placed posteriorly or inferiorly as these positions will fail to produce an anatomic reconstruction and exposes the popliteal neurovascular structures to injury (Figure 3) [43]. Clinical Outcomes of DB-PCL Reconstructions
Although anatomical and biomechanical studies have been successful in showing decreased posterior tibial translation and increased rotational stability following PCLR, outcomes studies have produced more equivocal results. A recent systematic review compared outcomes of nonoperative management and PCLR in isolated PCL injuries. Conservative management produced a success rate of 33% while surgical intervention resulted in a 90% success rate. Moreover, side to side difference as measured by Telos, ranged from 2.0 to 3.7 in the surgical group and from 3.5 to 5.3 in the nonoperative group. Lastly, and perhaps most importantly, the nonoperative group had more residual anterior-posterior laxity than the surgical group. The combination of these results allowed the study to conclude that surgical intervention produces more satisfactory and consistent stability [10]. Comparing the outcomes of SB-PCLR and DB-PCLR is important to ensure that the previously discussed anatomical superiority of the DB-PCLR indeed produces better biomechanical and clinical outcomes. A recent systematic review concluded that DB-PCLR was significantly superior over SB-PCLR from a biomechanical standpoint [14]. However, no significant difference was found between the two techniques with respect to clinical outcomes at this point in time [14]. Similarly, Harner et al. found the DB-PCLR to be biomechanically superior with regard to posterior tibial translation when they compared SB-PCLR to normal knees and DB-PCLR to normal knees [8]. These studies highlight the superior biomechanics and the lack of robust clinical outcomes following DB-PCLR.
Spiridonov et al. postulated that tech-nique variation may drive changes in clinical outcomes following DB-PCLR [44]. The majority of surgical approaches involve splitting the vastus medialis obliquus (VMO) via anterolateral portal placement, which may result in quadriceps muscle weakness. The study evaluated 31 patients with grade II PCL tears following VMO-sparing DB-PCL reconstruction. They use a transtibial reconstruction with Achilles allograft placed via a lateral arthroscopic portal [44]. Graft fixation was achieved through an all-inside method and secured distally though a transtibial tunnel, thus avoiding VMO injury. At a minimum of two years follow up, the authors reported significant improvements in subjective and objective outcomes. These findings reflect the capacity of the DB-PCLR to produce great clinical results, however more studies are needed to corroborate these findings.
CONCLUSIONS
Many recent studies have elucidated the anatomical and biomechanical properties of the PCL have led to new surgical techniques and innovation. More recent studies have help maximize the surgeon’s ability to produce anatomic reconstructions following PCL injury. Double bundle PCL reconstructions allow for optimal resistance to posterior tibial translation while also allowing for restoration of rotational stability. Thus far, short term outcomes are promising. However, future studies must focus on the long-term clinical efficacy of the DB-PCL reconstruction to ensure that it is superior from not only an anatomical and biomechanical standpoint, but also with respect to patient outcomes. REFERENCES
[1] Parolie JM, Bergfeld JA. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med. 1986;14(1):35-8.
[2] Torg JS, Barton TM, Pavlov H, Stine R.Natural history of the posterior cruciate ligament-deficient knee. Clin Ortho Rel Res. 1989;(246):208-26.
[3] Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ. Arthroscopic evaluation of articular cartilage lesions in posterior-cruciate-ligament-deficient knees. Arthroscopy. 2003;9(3):262-8.
[4] Van de Velde SK, Bingham JT, Gill TJ, Li G. Analysis of tibiofemoral cartilage deformation in the posterior cruciate ligament-deficient knee.J Bone Joint Surg (Am). 2009;91(1):167-75.
[5] McAllister DR, Petrigliano FA. Diagnosis and treatment of posterior cruciate ligament injuries. Curr Sports Med Rep. 2007;6(5):293-9.
[6] Sekiya JK, Whiddon DR, Zehms CT, Miller MD. A clinically relevant assessment of posterior cruciate ligament and posterolateral corner injuries. Evaluation of isolated and combined deficiency. J Bone Joint Surg (Am). 2008;90:1621-7.
[7] Papannagari R, DeFrate LE, Nha KW, Moses JM, Moussa M, Gill TJ, Li G. Function of posterior cruciate ligament bundles during in vivo knee flexion. Am J Sports Med. 2007;35:1507-12.
[8] Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28:144-51.
[9] Sanders TL, Pareek A, Barrett IJ, Kremers HM, Bryan AJ, Stuart MJ, Levy BA, Krych AJ. Incidence and long-term follow-up of isolated posterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 2016.
[10] Ahn S, Lee YS, Song YD, Chang CB, Kang SB, Choi YS. Does surgical reconstruction produce better stability than conservative treatment in the isolated PCL injuries? Arch Orthop Trauma Surg. 2016;136:811-9.
[11] Kennedy NI, LaPrade RF, Goldsmith MT, Faucett SC, Rasmussen MT, Coatney GA, Engebretsen L, Wijdicks CA. Posterior cruciate ligament graft fixation angles, part 1: biomechanical evaluation for anatomic single-bundle reconstruction. Am J Sports Med. 2014;42:2338-45.
[12] Lenschow S, Zantop T, Weimann A, Lemburg T, Raschke M, Strobel M, Petersen W. Joint kinematics and in situ forces after single bundle PCL reconstruction: a graft placed at the center of the femoral attachment does not restore normal posterior laxity. Arch Orthop Trauma Surg. 2006;126:253-9.
[13] Matava MJ, Ellis E, Gruber B. Surgical treatment of posterior cruciate ligament tears: an evolving technique. J Am Acad Orthop Surg. 17(7):435-6.
[14] Qi YS, Wang HJ, Wang SJ, Zhang ZZ, Huang AB, Yu JK. A systematic review of double-bundle versus single-bundle posterior cruciate ligament reconstruction. BMC Musculoskelet Disord. 2016;17:45.
[15] Parolie JM, Bergfeld JA. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med , 1986, 14(1):35-8.
[16] Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Ortho Rel Res, 1975(106):216-31.
[17] Harner CD, Xerogeanes JW, Livesay GA, Carlin GJ, Smith BA, Kusayama T, Kashiwaguchi S, Woo SL. The human posterior cruciate ligament complex: an interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med, 1995;23(6):736-45.
[18] Race A, Amis AA. The mechanical properties of the two bundles of the human posterior cruciate ligament. J Biomech. 1994;27(1):13-24.
[19] Kennedy JC, Hawkins RJ, Willis RB, Danylchuck KD. Tension studies of human knee ligaments. Yield point, ultimate failure, and disruption of the cruciate and tibial collateral ligaments. J Bone J Surg (Am), 1976, 58(3):350-5.
[20] Gupte CM, Bull AM, Thomas RD, Amis AA. A review of the function and biomechanics of the meniscofemoral ligaments. Arthroscopy. 2003;19:161-71.
[21] Markolf KL, Feeley BT, Tejwani SG, Martin DE, McAllister DR: Changes in knee laxity and ligament force after sectioning the posteromedial bundle of the posterior cruciate ligament. Arthroscopy. 2006;22(10):1100-6.
[22] Markolf KL, Zemanovic JR, McAllister DR. Cyclic loading of posterior cruciate ligament replacements fixed with tibial tunnel and tibial inlay methods. J Bone Joint Surg (Am). 2002;84A:518-24.
[23] Kennedy NI, Wijdicks CA, Goldsmith MT, Michalski MP, Devitt BM, Aroen A, Engebretsen L, LaPrade RF. Kinematic analysis of the posterior cruciate ligament, part 1: the individual and collective function of the anterolateral and posteromedial bundles. Am J Sports Med. 2013;41:2828-38.
[24] Escamilla RF, Zheng N, MacLeod TD, Imamura R, Edwards WB, Hreljac A, Fleisig GS, Wilk KE, Moorman CT, Paulos L, Andrews JR. Cruciate ligament tensile forces during the forward and side lunge. Clin Biomech. 2010;25:213-21.
[25] Jeong WS, Yoo YS, Kim DY, Shetty NS, Smolinski P, Logishetty K, Ranawat A. An analysis of the posterior cruciate ligament isometric position using an in vivo 3-dimensional computed tomography-based knee joint model. Arthroscopy. 2010;26:1333-9.
[26] Li G, DeFrate LE, Sun H, Gill TJ. In vivo elongation of the anterior cruciate ligament and posterior cruciate ligament during knee flexion. Am J Sports Med. 2004;32:1415-20.
[27] Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles. An analysis of bundle lengths and orientation. Am J Sports Med. 2003;31:221-5.
[28] Wijdicks CA, Kennedy NI, Goldsmith MT, Devitt BM, Michalski MP, Aroen A, Engebretsen L, LaPrade RF. Kinematic analysis of the posterior cruciate ligament, part 2: a comparison of anatomic single- versus double-bundle reconstruction. Am J Sports Med. 2013;41(12):2839-48.
[29] Owesen C, Sandven-Thrane S, Lind M, Forssblad M, Granan LP, Aroen A. Epidemiology of surgically treated posterior cruciate ligament injuries in Scandinavia. Knee Surg Sports Traumatol Arthrosc. 2015. [30] Kozanek M, Fu EC, Van de Velde SK, Gill TJ, Li G. Posterolateral structures of the knee in posterior cruciate ligament deficiency. Am J Sports Med. 2009;37:534-41.
[31] Moulton SG, Cram TR, James EW, Dornan GJ, Kennedy NI, LaPrade RF. The Supine Internal Rotation Test: A Pilot Study Evaluating Tibial Internal Rotation in Grade III Posterior Cruciate Ligament Tears. Orthop J Sports Med. 2015;3(2):2325967115572135.
[32] Jackman T, LaPrade RF, Pontinen T, Lender PA. Intraobserver and interobserver reliability of the kneeling technique of stress radiography for the evaluation of posterior knee laxity. Am J Sports Med. 2008; 36(8):1571-6.
[33] Allen CR RJ, Harner CD. Posterior cruciate ligament: diagnosis and decision making. In Miller MD, Cole BJ (Eds), Textbook of Arthroscopy 2004, Elsevier.
[34] Jung YB, Tae SK, Lee YS, Jung HJ, Nam CH, Park SJ. Active nonoperative treatment of acute isolated posterior cruciate ligament injury with cylinder cast immobilization. Knee Surg Sports Traumatol Arthrosc. 2008;16:729-33.
[35] LaPrade RF, Smith SD, Wilson KJ, Wijdicks CA. Quantification of functional brace forces for posterior cruciate ligament injuries on the knee joint: an in vivo investigation. Knee Surg Sports Traumatol Arthrosc. 2015;23:3070-6.
[36] Sekiya JK, West RV, Ong BC, Irrgang JJ, Fu FH, Harner CD. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2005;21:1042-50.
[37] Mejia EA, Noyes FR, Grood ES. Posterior cruciate ligament femoral insertion site characteristics. Importance for reconstructive procedures. Am J Sports Med. 2002;30:643-51.
[38] Edwards A, Bull AM, Amis AA: The attachments of the fiber bundles of the posterior cruciate ligament: an anatomic study. Arthroscopy. 2007;23(3):284-90.
[39] Anderson CJ, Ziegler CG, Wijkicks CA, Engebretsen L, LaPrade RF. Arthroscopically pertinent anatomy of the anterolateral and posteromedial bundles of the posterior cruciate ligament. J Bone Joint Surg (Am). 2012;94(21):1936-45.
[40] Lutz GE, Palmitier RA, An KN, Chao EY: Comparison of tibiofemoral joint forces during open-kinetic-chain and closed-kinetic-chain exercises. J Bone J Surg (Am). 1993;75(5):732-9.
[41] Apsingi S, Bull AM, Deehan DJ, Amis AA. Review: femoral tunnel placement for PCL reconstruction in relation to the PCL fibre bundle attachments. Knee Surg Sports Traumatol Arthrosc. 2009;17:652-9.
[42] Harner CD, Baek GH, Vogrin TM, Carlin GJ, Kashiwaguchi S, Woo SL. Quantitative analysis of human cruciate ligament insertions. Arthroscopy. 1999;15:741-9.
[43] Kennedy NI, Michalski MP, Engebretsen L, LaPrade RF. Iatrogenic Meniscus Posterior Root Injury Following Reconstruction of the Posterior Cruciate Ligament. A Report of Three Cases. JBJS Case Connect 2014;4:e20.
[44] Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle reconstruction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg (Am). 2011;93:1773-80.
Many recent studies have elucidated the anatomical and biomechanical properties of the PCL have led to new surgical techniques and innovation. More recent studies have help maximize the surgeon’s ability to produce anatomic reconstructions following PCL injury. Double bundle PCL reconstructions allow for optimal resistance to posterior tibial translation while also allowing for restoration of rotational stability. Thus far, short term outcomes are promising. However, future studies must focus on the long-term clinical efficacy of the DB-PCL reconstruction to ensure that it is superior from not only an anatomical and biomechanical standpoint, but also with respect to patient outcomes. REFERENCES
[1] Parolie JM, Bergfeld JA. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med. 1986;14(1):35-8.
[2] Torg JS, Barton TM, Pavlov H, Stine R.Natural history of the posterior cruciate ligament-deficient knee. Clin Ortho Rel Res. 1989;(246):208-26.
[3] Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ. Arthroscopic evaluation of articular cartilage lesions in posterior-cruciate-ligament-deficient knees. Arthroscopy. 2003;9(3):262-8.
[4] Van de Velde SK, Bingham JT, Gill TJ, Li G. Analysis of tibiofemoral cartilage deformation in the posterior cruciate ligament-deficient knee.J Bone Joint Surg (Am). 2009;91(1):167-75.
[5] McAllister DR, Petrigliano FA. Diagnosis and treatment of posterior cruciate ligament injuries. Curr Sports Med Rep. 2007;6(5):293-9.
[6] Sekiya JK, Whiddon DR, Zehms CT, Miller MD. A clinically relevant assessment of posterior cruciate ligament and posterolateral corner injuries. Evaluation of isolated and combined deficiency. J Bone Joint Surg (Am). 2008;90:1621-7.
[7] Papannagari R, DeFrate LE, Nha KW, Moses JM, Moussa M, Gill TJ, Li G. Function of posterior cruciate ligament bundles during in vivo knee flexion. Am J Sports Med. 2007;35:1507-12.
[8] Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28:144-51.
[9] Sanders TL, Pareek A, Barrett IJ, Kremers HM, Bryan AJ, Stuart MJ, Levy BA, Krych AJ. Incidence and long-term follow-up of isolated posterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 2016.
[10] Ahn S, Lee YS, Song YD, Chang CB, Kang SB, Choi YS. Does surgical reconstruction produce better stability than conservative treatment in the isolated PCL injuries? Arch Orthop Trauma Surg. 2016;136:811-9.
[11] Kennedy NI, LaPrade RF, Goldsmith MT, Faucett SC, Rasmussen MT, Coatney GA, Engebretsen L, Wijdicks CA. Posterior cruciate ligament graft fixation angles, part 1: biomechanical evaluation for anatomic single-bundle reconstruction. Am J Sports Med. 2014;42:2338-45.
[12] Lenschow S, Zantop T, Weimann A, Lemburg T, Raschke M, Strobel M, Petersen W. Joint kinematics and in situ forces after single bundle PCL reconstruction: a graft placed at the center of the femoral attachment does not restore normal posterior laxity. Arch Orthop Trauma Surg. 2006;126:253-9.
[13] Matava MJ, Ellis E, Gruber B. Surgical treatment of posterior cruciate ligament tears: an evolving technique. J Am Acad Orthop Surg. 17(7):435-6.
[14] Qi YS, Wang HJ, Wang SJ, Zhang ZZ, Huang AB, Yu JK. A systematic review of double-bundle versus single-bundle posterior cruciate ligament reconstruction. BMC Musculoskelet Disord. 2016;17:45.
[15] Parolie JM, Bergfeld JA. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med , 1986, 14(1):35-8.
[16] Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Ortho Rel Res, 1975(106):216-31.
[17] Harner CD, Xerogeanes JW, Livesay GA, Carlin GJ, Smith BA, Kusayama T, Kashiwaguchi S, Woo SL. The human posterior cruciate ligament complex: an interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med, 1995;23(6):736-45.
[18] Race A, Amis AA. The mechanical properties of the two bundles of the human posterior cruciate ligament. J Biomech. 1994;27(1):13-24.
[19] Kennedy JC, Hawkins RJ, Willis RB, Danylchuck KD. Tension studies of human knee ligaments. Yield point, ultimate failure, and disruption of the cruciate and tibial collateral ligaments. J Bone J Surg (Am), 1976, 58(3):350-5.
[20] Gupte CM, Bull AM, Thomas RD, Amis AA. A review of the function and biomechanics of the meniscofemoral ligaments. Arthroscopy. 2003;19:161-71.
[21] Markolf KL, Feeley BT, Tejwani SG, Martin DE, McAllister DR: Changes in knee laxity and ligament force after sectioning the posteromedial bundle of the posterior cruciate ligament. Arthroscopy. 2006;22(10):1100-6.
[22] Markolf KL, Zemanovic JR, McAllister DR. Cyclic loading of posterior cruciate ligament replacements fixed with tibial tunnel and tibial inlay methods. J Bone Joint Surg (Am). 2002;84A:518-24.
[23] Kennedy NI, Wijdicks CA, Goldsmith MT, Michalski MP, Devitt BM, Aroen A, Engebretsen L, LaPrade RF. Kinematic analysis of the posterior cruciate ligament, part 1: the individual and collective function of the anterolateral and posteromedial bundles. Am J Sports Med. 2013;41:2828-38.
[24] Escamilla RF, Zheng N, MacLeod TD, Imamura R, Edwards WB, Hreljac A, Fleisig GS, Wilk KE, Moorman CT, Paulos L, Andrews JR. Cruciate ligament tensile forces during the forward and side lunge. Clin Biomech. 2010;25:213-21.
[25] Jeong WS, Yoo YS, Kim DY, Shetty NS, Smolinski P, Logishetty K, Ranawat A. An analysis of the posterior cruciate ligament isometric position using an in vivo 3-dimensional computed tomography-based knee joint model. Arthroscopy. 2010;26:1333-9.
[26] Li G, DeFrate LE, Sun H, Gill TJ. In vivo elongation of the anterior cruciate ligament and posterior cruciate ligament during knee flexion. Am J Sports Med. 2004;32:1415-20.
[27] Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles. An analysis of bundle lengths and orientation. Am J Sports Med. 2003;31:221-5.
[28] Wijdicks CA, Kennedy NI, Goldsmith MT, Devitt BM, Michalski MP, Aroen A, Engebretsen L, LaPrade RF. Kinematic analysis of the posterior cruciate ligament, part 2: a comparison of anatomic single- versus double-bundle reconstruction. Am J Sports Med. 2013;41(12):2839-48.
[29] Owesen C, Sandven-Thrane S, Lind M, Forssblad M, Granan LP, Aroen A. Epidemiology of surgically treated posterior cruciate ligament injuries in Scandinavia. Knee Surg Sports Traumatol Arthrosc. 2015. [30] Kozanek M, Fu EC, Van de Velde SK, Gill TJ, Li G. Posterolateral structures of the knee in posterior cruciate ligament deficiency. Am J Sports Med. 2009;37:534-41.
[31] Moulton SG, Cram TR, James EW, Dornan GJ, Kennedy NI, LaPrade RF. The Supine Internal Rotation Test: A Pilot Study Evaluating Tibial Internal Rotation in Grade III Posterior Cruciate Ligament Tears. Orthop J Sports Med. 2015;3(2):2325967115572135.
[32] Jackman T, LaPrade RF, Pontinen T, Lender PA. Intraobserver and interobserver reliability of the kneeling technique of stress radiography for the evaluation of posterior knee laxity. Am J Sports Med. 2008; 36(8):1571-6.
[33] Allen CR RJ, Harner CD. Posterior cruciate ligament: diagnosis and decision making. In Miller MD, Cole BJ (Eds), Textbook of Arthroscopy 2004, Elsevier.
[34] Jung YB, Tae SK, Lee YS, Jung HJ, Nam CH, Park SJ. Active nonoperative treatment of acute isolated posterior cruciate ligament injury with cylinder cast immobilization. Knee Surg Sports Traumatol Arthrosc. 2008;16:729-33.
[35] LaPrade RF, Smith SD, Wilson KJ, Wijdicks CA. Quantification of functional brace forces for posterior cruciate ligament injuries on the knee joint: an in vivo investigation. Knee Surg Sports Traumatol Arthrosc. 2015;23:3070-6.
[36] Sekiya JK, West RV, Ong BC, Irrgang JJ, Fu FH, Harner CD. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2005;21:1042-50.
[37] Mejia EA, Noyes FR, Grood ES. Posterior cruciate ligament femoral insertion site characteristics. Importance for reconstructive procedures. Am J Sports Med. 2002;30:643-51.
[38] Edwards A, Bull AM, Amis AA: The attachments of the fiber bundles of the posterior cruciate ligament: an anatomic study. Arthroscopy. 2007;23(3):284-90.
[39] Anderson CJ, Ziegler CG, Wijkicks CA, Engebretsen L, LaPrade RF. Arthroscopically pertinent anatomy of the anterolateral and posteromedial bundles of the posterior cruciate ligament. J Bone Joint Surg (Am). 2012;94(21):1936-45.
[40] Lutz GE, Palmitier RA, An KN, Chao EY: Comparison of tibiofemoral joint forces during open-kinetic-chain and closed-kinetic-chain exercises. J Bone J Surg (Am). 1993;75(5):732-9.
[41] Apsingi S, Bull AM, Deehan DJ, Amis AA. Review: femoral tunnel placement for PCL reconstruction in relation to the PCL fibre bundle attachments. Knee Surg Sports Traumatol Arthrosc. 2009;17:652-9.
[42] Harner CD, Baek GH, Vogrin TM, Carlin GJ, Kashiwaguchi S, Woo SL. Quantitative analysis of human cruciate ligament insertions. Arthroscopy. 1999;15:741-9.
[43] Kennedy NI, Michalski MP, Engebretsen L, LaPrade RF. Iatrogenic Meniscus Posterior Root Injury Following Reconstruction of the Posterior Cruciate Ligament. A Report of Three Cases. JBJS Case Connect 2014;4:e20.
[44] Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle reconstruction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg (Am). 2011;93:1773-80.