Two-Stage Revision for a Chronic Prosthetic Infection of a Megaprosthesis
Travis L. Anthony, MD; Russel A. Ward, MD
Department of Orthopaedic Surgery, Baylor Scott & White Health; Temple, TX, USA
Corresponding Author:Travis L. Anthony, MD, Department of Orthopaedic Surgery, Baylor Scott & White Health, 2401 S. 31st St., Temple, TX 76508, USA; travis.anthony@BSWHealth.org
DOI: 10.18600/toj.0201114
INTRODUCTION
Limb salvage procedures for high-grade sarcomas have become the standard of care in many patients undergoing operative resection. Studies have continued to show that limb salvage procedures provide disease-free intervals similar to amputations [1,2], and most patients achieve a good functional outcome [2,3]. While these results have been encouraging, the use of an endoprosthesis for limb salvage procedures poses its own set of difficulties. Implants have a limited lifespan in an oftentimes young patient population. Combine this with the risk of periprosthetic fractures and infections, and reoperation rates remain a real problem in these patients. Infection is a serious and unfortunately common problem, with rates being reported with the use of a megaprosthesis ranging from 3-31% [4]. Following an infection, the ability to perform a staged limb salvage revision procedure has been directly correlated with the condition of the surrounding soft tissues [5]. The patient described in this case report is an example of such a case where a novel technique was utilized to preserve the soft-tissue envelope around a megaprosthesis, thus allowing for a successful 2-stage revision.
Limb salvage procedures for high-grade sarcomas have become the standard of care in many patients undergoing operative resection. Studies have continued to show that limb salvage procedures provide disease-free intervals similar to amputations [1,2], and most patients achieve a good functional outcome [2,3]. While these results have been encouraging, the use of an endoprosthesis for limb salvage procedures poses its own set of difficulties. Implants have a limited lifespan in an oftentimes young patient population. Combine this with the risk of periprosthetic fractures and infections, and reoperation rates remain a real problem in these patients. Infection is a serious and unfortunately common problem, with rates being reported with the use of a megaprosthesis ranging from 3-31% [4]. Following an infection, the ability to perform a staged limb salvage revision procedure has been directly correlated with the condition of the surrounding soft tissues [5]. The patient described in this case report is an example of such a case where a novel technique was utilized to preserve the soft-tissue envelope around a megaprosthesis, thus allowing for a successful 2-stage revision.
CASE REPORT
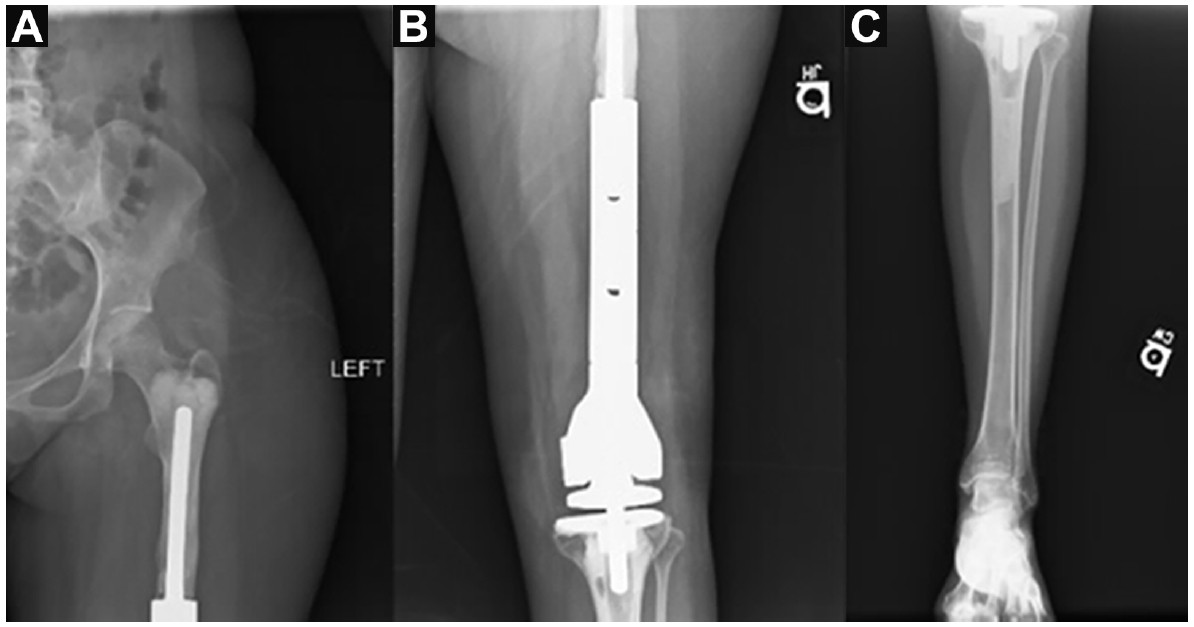
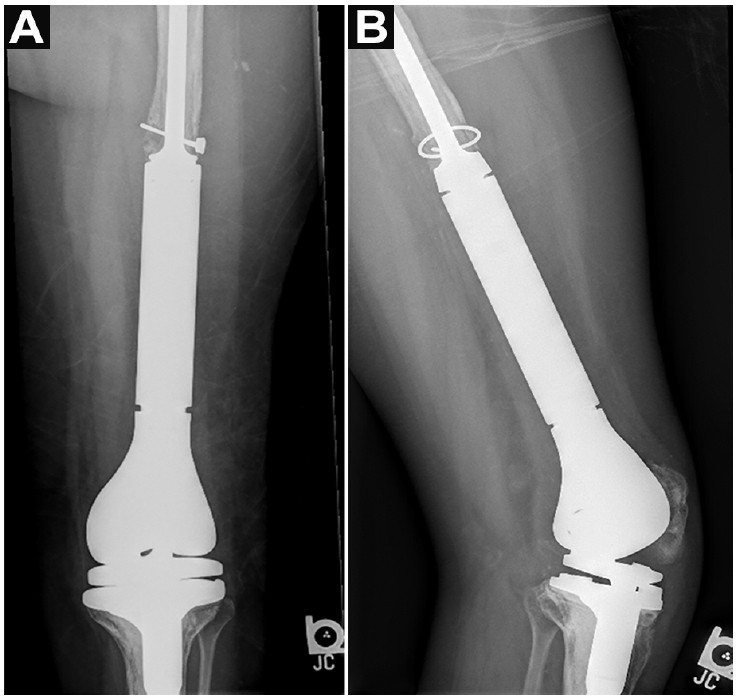
The patient is a 33-year-old Hispanic female with an extensive 20-year orthopedic history beginning at the age of 13 when she was diagnosed with an osteosarcoma of her left distal femur. An expandable prosthesis was surgically placed, which was subsequently replaced with a rotating hinge tumor prosthesis. Since that time, the patient has had 2 additional revisions due to a loosening of the prosthesis. Most recently, while out of the country, she fell and suffered a hemarthrosis, which led to the suggestion that she should have immediate surgery. A lateral parapatellar arthrotomy resulted in surgical drainage and removal or portions of the hardware. The patient presented to the emergency department of our facility with complaints of pain and swelling about the knee following 2 hyperflexion injuries over the last 2 months following her last surgery (Figure 1). No complaints of fever, chills, nausea, or vomiting were noted at the time. Lab results revealed a white blood cell count of 8,100 x 109/L, a C-reactive protein of 16.8 mg/L, and erythrocyte sedimentation rate of 53 mm/hour. A physical exam showed passive range of motion ranging from full extension to 45 degrees of flexion.
The patient is a 33-year-old Hispanic female with an extensive 20-year orthopedic history beginning at the age of 13 when she was diagnosed with an osteosarcoma of her left distal femur. An expandable prosthesis was surgically placed, which was subsequently replaced with a rotating hinge tumor prosthesis. Since that time, the patient has had 2 additional revisions due to a loosening of the prosthesis. Most recently, while out of the country, she fell and suffered a hemarthrosis, which led to the suggestion that she should have immediate surgery. A lateral parapatellar arthrotomy resulted in surgical drainage and removal or portions of the hardware. The patient presented to the emergency department of our facility with complaints of pain and swelling about the knee following 2 hyperflexion injuries over the last 2 months following her last surgery (Figure 1). No complaints of fever, chills, nausea, or vomiting were noted at the time. Lab results revealed a white blood cell count of 8,100 x 109/L, a C-reactive protein of 16.8 mg/L, and erythrocyte sedimentation rate of 53 mm/hour. A physical exam showed passive range of motion ranging from full extension to 45 degrees of flexion.
Actively, she had approximately 10 degrees of extensor lag; however, she maintained 45 degrees of flexion. No evidence of valgus, varus, anterior, or posterior instability was observed at the hinged interface. An aspiration from the left knee was attempted, yielding 1 cc of bloody fluid. Synovial analysis showed a red fluid containing 20 million red blood cells and 2,000 white blood cells; 16% were neutrophils, 78% were lymphocytes, and 6 % were monocytes. Cultures of the synovial aspirate confirmed the presence of Staphylococcus lugdunensis. Follow-up labs were obtained 3 days after the initial visit and revealed a white blood cell count of 8,000 x 109/L and a C-reactive protein of 26.1 mg/L. After discussing options with the patient and her family, it was determined the best course of action was to perform a 2-stage revision with an interim antibiotic spacer.
The previous extensile left lateral parapatellar approach was again utilized. After careful dissection, the distal femur prosthesis was encountered and was circumferentially dissected. Purulence was noticed over the proximal portion of the distal femur component. Once circumferential dissection was achieved around the proximal tibia, the hinge was disarticulated. The proximal junction of the distal femur modular component was disarticulated using a standard spreader device.
The previous extensile left lateral parapatellar approach was again utilized. After careful dissection, the distal femur prosthesis was encountered and was circumferentially dissected. Purulence was noticed over the proximal portion of the distal femur component. Once circumferential dissection was achieved around the proximal tibia, the hinge was disarticulated. The proximal junction of the distal femur modular component was disarticulated using a standard spreader device.

During disarticulation of the extension piece of the prosthesis from the stem, it was found that the stem was loose at the cement implant interface. The stem was then tamped out of the cement implant interface leaving the cement behind. The rotating hinge tibial component was removed piecemeal. The remaining cement in the proximal tibia was meticulously removed using a series of osteotomes, curettes, and an ultrasonic cement extractor. The cement in the proximal femur was intentionally not removed, accepting the risk of ongoing bacterial contamination due to the fact that its removal would potentially require conversion to a total femur replacement. After all components and tibial cement had been removed, a meticulous irrigation and debridement was performed. A spacer was fabricated on the back table. The cement recipe included 4 bags of bone cement with 3 g vancomycin powder and 3.6 g tobramycin powder.
The fabrication of the spacer was performed in 2 steps, creating a tibial stem and the distal femur component. The tibial stem was constructed used a 40-French chest tube as a mold. Bone cement was injected into the chest tube and allowed to harden to the late doughy phase, at which time a stainless steel Harrington rod was inserted for reinforcement.
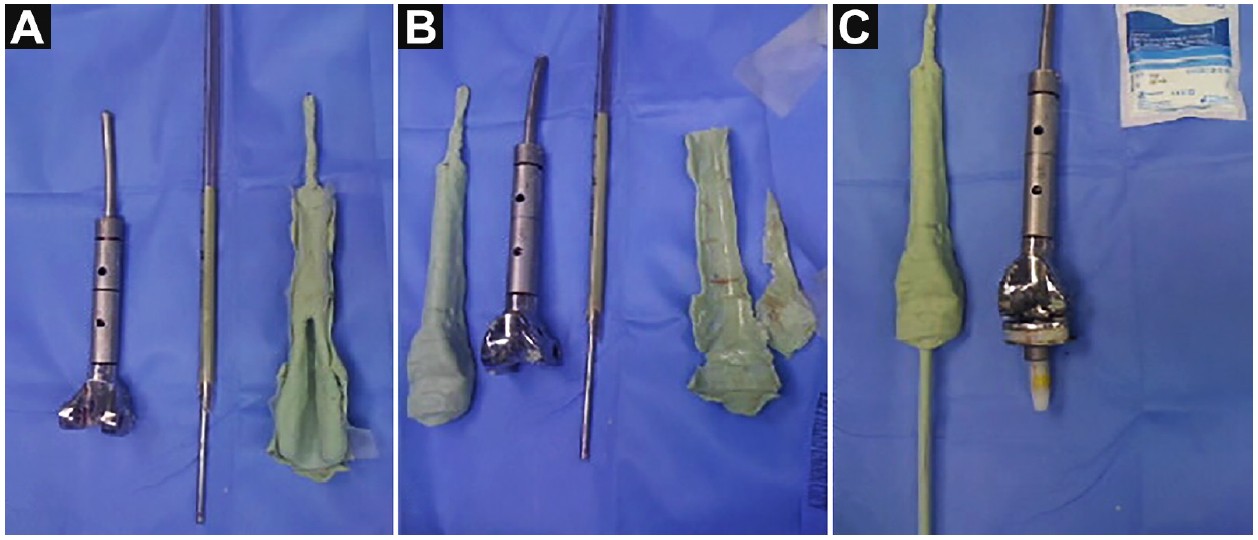
After the bone cement hardened, the tube was cut away, leaving the reinforced tibial component. The second step in the formation of the spacer was to construct the distal femur component of the endoprosthesis. To create an exact match of the removed hardware, bone cement was used to form a mold (Figures 2 and 3). This mold was used to create a custom distal femur component with contours matching the previous implant, with the goal of adequately maintaining the tissue envelope for the second stage of the revision. A nonadhesive petroleum mesh was utilized to prevent the spacer from sticking to the mold. Cement was placed in the mold along with a 3/16 inch Steinmann pin for stabilization. When the spacer reached the desired consistency, it was removed. We found 2 steps in the formation of this spacer that were critical for proper articulation: creating a tunnel in the femoral component for the spinal rod, and creating a trough in the distal aspect to allow for easier insertion of the femoral and tibial components.
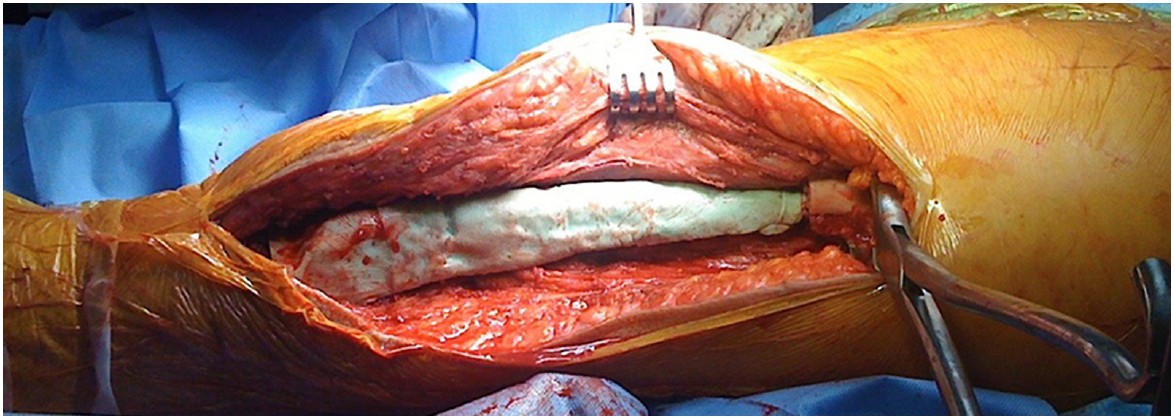
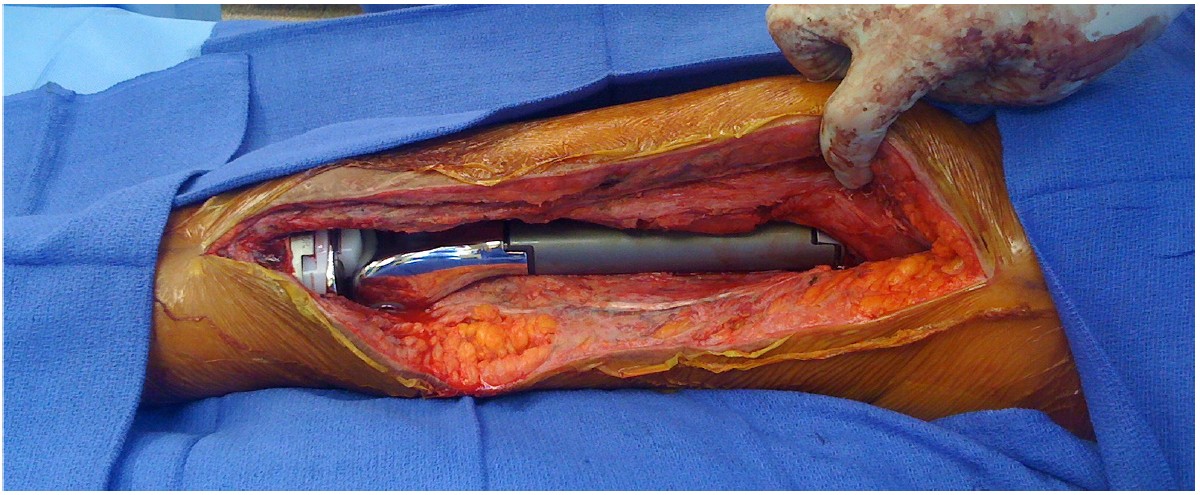
Articulation of the 2 components of the spacer was achieved by tamping the tibial component into place distally and the Steinmann pin portion of the femoral component into the femoral medullary cavity proximally. The proximal aspect of the tibial rod was then laid into the trough of the femoral component and inserted into the tunnel we created. An additional bag of bone cement was then mixed to secure the spacer into place by filling in the trough in the femoral component as well as the bone spacer interfaces to provide moderate stability for the duration of antibiotic spacing (Figure 4). The wound was again irrigated, and a multilayered closure was performed. Final images of the articulated spacer are demonstrated in Figure 5.

After a total duration of 2 months and a 6-week course of parenteral antibiotic therapy, the patient was successfully reimplanted and went on to heal uneventfully (Figure 6). At the last follow-up at 20-month status post re-implantation, the patient retained the prosthesis with good function including active motion from -5 to 90 degrees, and ambulated without an assistive device.
DISCUSSION
The patient presented is an example of the challenge that is often presented with treating osteosarcomas with limb salvage procedures. Multiple revision surgeries had been performed prior to the described operation, thus already compromising arguably the most important component of a 2-stage revision—the soft tissue envelope. This is a common occurrence among patients treated with megaendoprostheses with the average reoperation rate for these patients being reported at 2.6 procedures. However, with the use of a custom molded antibiotic spacer in this case, the difficulty level in performing the second stage of the revision was made significantly less.
Following the administration of long-term IV antibiotics, the patient returned to the OR for the second stage of her revision. The antibiotic spacer was removed and a new prosthesis was implanted. A medial release of the quadriceps musculature was utilized, thus allowing lateral excursion of the soft tissues and ultimately a loose closure. At the time of this paper, the patient had 2-year follow-up with infection control, and no evidence of hardware complications or soft-tissue breakdown (Figure 7).
The patient presented is an example of the challenge that is often presented with treating osteosarcomas with limb salvage procedures. Multiple revision surgeries had been performed prior to the described operation, thus already compromising arguably the most important component of a 2-stage revision—the soft tissue envelope. This is a common occurrence among patients treated with megaendoprostheses with the average reoperation rate for these patients being reported at 2.6 procedures. However, with the use of a custom molded antibiotic spacer in this case, the difficulty level in performing the second stage of the revision was made significantly less.
Following the administration of long-term IV antibiotics, the patient returned to the OR for the second stage of her revision. The antibiotic spacer was removed and a new prosthesis was implanted. A medial release of the quadriceps musculature was utilized, thus allowing lateral excursion of the soft tissues and ultimately a loose closure. At the time of this paper, the patient had 2-year follow-up with infection control, and no evidence of hardware complications or soft-tissue breakdown (Figure 7).
CONCLUSIONS
This case demonstrates some of the unique complexities in treating high-grade sarcomas with limb salvage procedures. Owing to the high complication and reoperation rates associated with such operations, one must be prepared to deal with these situations as they arise. In the specific case of an infected megaprosthesis where a 2-stage operation is required, the surgeon could consider using the previous implant as a mold for the antibiotic spacer to ensure adequate spacing. Using bone cement, this is a quick and simple technique to provide a close match to the native prosthesis. By doing so, the soft tissue envelope is preserved, which has been shown to be an important aspect in limb salvage revision surgeries. REFERENCES
[1] Simon MA, Aschliman MA, Thomas N, Mankin HJ. Limb-salvage treatment versus amputation for osteosarcoma of the distal end of the femur. J Bone Joint Surg Am. 1986;68(9):1331-7.
[2] Rougraff BT, Simon MA, Kneisl JS, Greenberg DB, Mankin HJ. Limb salvage compared with amputation for osteosarcoma of the distal end of the femur. A long term oncological, functional, and quality-of-life study. J Bone Joint Surg Am. 1994;76(5):649-56.
[3] Ottaviani G, Robert RS, Huh WW, Jaffe N. Functional, psychosocial, and professional outcomes in long-term survivors of lower extremity osteosarcomas: amputation versus limb salvage. Cancer Treat Res. 2009;152:421-36.
[4] Pilge H, Gradl G, von Eisenhart-Rothe R, Gollwitzer H. Incidence and outcome after infection of megaprostheses. Hip Int. 2012;22(Suppl 8):S83-90.
[5] Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, Gosheger G. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg. 2006;126(5):289-96.
This case demonstrates some of the unique complexities in treating high-grade sarcomas with limb salvage procedures. Owing to the high complication and reoperation rates associated with such operations, one must be prepared to deal with these situations as they arise. In the specific case of an infected megaprosthesis where a 2-stage operation is required, the surgeon could consider using the previous implant as a mold for the antibiotic spacer to ensure adequate spacing. Using bone cement, this is a quick and simple technique to provide a close match to the native prosthesis. By doing so, the soft tissue envelope is preserved, which has been shown to be an important aspect in limb salvage revision surgeries. REFERENCES
[1] Simon MA, Aschliman MA, Thomas N, Mankin HJ. Limb-salvage treatment versus amputation for osteosarcoma of the distal end of the femur. J Bone Joint Surg Am. 1986;68(9):1331-7.
[2] Rougraff BT, Simon MA, Kneisl JS, Greenberg DB, Mankin HJ. Limb salvage compared with amputation for osteosarcoma of the distal end of the femur. A long term oncological, functional, and quality-of-life study. J Bone Joint Surg Am. 1994;76(5):649-56.
[3] Ottaviani G, Robert RS, Huh WW, Jaffe N. Functional, psychosocial, and professional outcomes in long-term survivors of lower extremity osteosarcomas: amputation versus limb salvage. Cancer Treat Res. 2009;152:421-36.
[4] Pilge H, Gradl G, von Eisenhart-Rothe R, Gollwitzer H. Incidence and outcome after infection of megaprostheses. Hip Int. 2012;22(Suppl 8):S83-90.
[5] Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, Gosheger G. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg. 2006;126(5):289-96.