Bone Contact of a Straight versus an Angled Tibiotalocalcaneal Arthrodesis Intramedullary Nail
Shelton McKenzie, MD¹; Domingo Molina, MD²; Randal P. Morris, BS³; Vinod K. Panchbhavi MD³
¹Orthopaedic Surgery & Rehabilitation, Howard University Hospital; Washington, DC, USA²Department of Orthopaedics & Sports Medicine, University of Kentucky; Lexington, KY, USA³Department of Orthopaedic Surgery & Rehabilitation; University of Texas Medical Branch; Galveston, TX, USA
Corresponding Author:Vinod K. Panchbhavi, MD, FACS, Department of Orthopaedic Surgery & Rehabilitation, University of Texas Medical Branch, 301 University Blvd., Galveston, TX 77555; USA; vkpanchb@utmb.edu
DOI: 10.18600/toj.020109
INTRODUCTION
Tibiotalocalcaneal arthrodesis has become an increasingly popular procedure. The use of intramedullary nailing is beneficial for subtalar and tibiotalar arthritis, posttraumatic injury, as well as a salvage technique for previous failed surgery [1]. One method of achieving this arthrodesis is with the use of an intramedullary nail passed in a retrograde fashion. The intramedullary nail construct has proven to provide biomechanical stiffness in all bending and rotational directions [2]. The majority of intramedullary nails used for tibiocalcaneal arthrodesis are straight in design. However, it has been documented that straight nails often have very little purchase in the calcaneus, often engaging only the sustentaculum tali [3]. This limitation diminishes the calcaneal bone-to-rod interface and thus the stability.
Recent advances in nail design have produced nails with valgus and posterior curves. Previous studies have shown that a nail with a single lateral curve occupies more volume in the calcaneus than a straight nail [4]. However, to our knowledge, there is no report comparing a nail with a distal lateral and posterior bend with the surface area occupied by a straight nail. The purpose of this investigation is to compare the surface area of calcaneal bone contact with a straight nail versus a curved nail with a valgus and posterior bend. MATERIALS & METHODS
Nail Insertion
Seven pairs of embalmed cadaver legs stored at -4°C were thawed at room temperature 12 hours prior to preparation and dissection. The specimens had no visible pathology or deformity and were selected randomly for nail fixation. Each specimen was sectioned at the level of the isthmus to ensure the narrowest of diameters in the tibial shaft. While in contradiction to clinical practice, the joint surfaces were not prepared. This method follows previous cadaveric studies by McGarvey et al. [3] and Pochatko et al. [5]. It is believed that it is easier to hold the correct position of the unprepared specimen and the relationship between the talus and tibia would be unchanged compared to a prepared joint. The foot was then placed in 2-5 degrees of valgus, 90 degrees of foot-to-tibial shaft dorsiflexion, and approximately 10 degrees of external rotation [3]. The position was held in place manually to simulate standard operative techniques. In 1 limb of each pair, a straight nail preparation design was implanted (Orthofix Ankle Compression Nail, Orthofix; Verona, Italy). A 3-mm-diameter Kirschner guide wire was placed in an antegrade fashion through the center of the tibia, through the talus, and into the calcaneus. A rigid 13-mm entry reamer was then used to ream the path for the nail in an antegrade fashion. In the contralateral limb from each pair, a curved nail preparation design was implanted (A3-Anatomic Ankle Arthrodesis System Nail, Small Bone Innovations; Berlin, Germany). This intramedullary nail design includes a distal double bend, 1 posterior and 1 lateral. Adjustments were required for insertion of the curved nail to account for the posterior and lateral curve. First, a 3-mm diameter Kirschner guide wire was placed antegrade through the calcaneus, similar to the straight nail insertion. An offset guide was placed and aligned with the second ray. Using the system-aiming design, a second guide wire was placed through the offset guide in an antegrade fashion to account for the posterolateral curve of the nail. The 13-mm-diameter entry reamer was then passed over the second guide wire in a retrograde fashion across the calcaneus and talus. Reaming was performed by the same person for each paired specimen. The use of a 13-mm reamer was used for both nail designs to account for the 13-mm standard distal diameter of the curved nail design.
Determining Surface Area Bone Contact
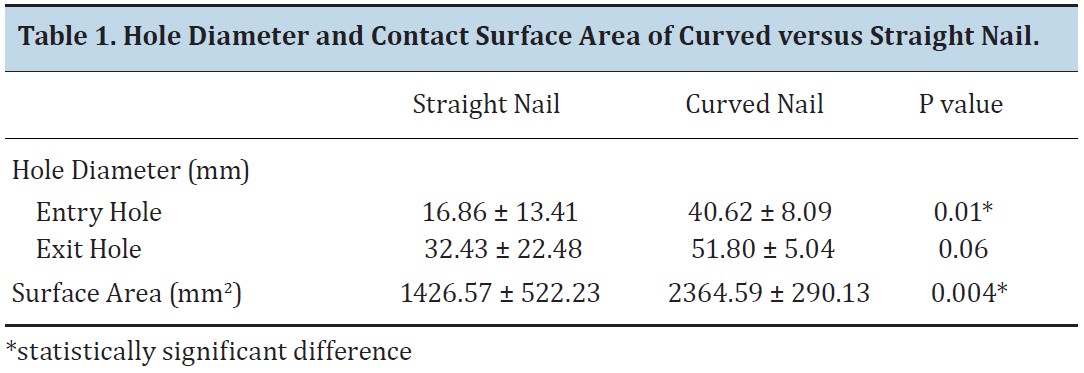
After reaming in both paired limbs, soft tissue dissection was performed and the calcaneus was disarticulated from the tibia and talus. The diameters of the entry and exit sites for each calcaneus were recorded and used to calculate the surface area of the cylindrical shape created by reaming. A 3-dimensional digitizer (MicroScribe 3DX, Immersion Corporation; San Jose, CA) and 3-dimensional surface reconstruction software was used to manually digitize the circumference of the entry and exit points reamed in the calcaneus. A 3-dimensional model of the bone in contact with the hindfoot nail was accomplished by triangulating points between entry and exit points in the calcaneus using the digitizer. Surface area was then calculated with a positional accuracy of 0.23 mm. Paired t-tests were used to determine whether the observed differences between the straight and curved nail were significant, with the level of significance set at 0.05. RESULTS The entry and exit diameters for each calcaneus used to calculate the surface area of bone contact are depicted in Table 1. The mean surface area for the straight nail design was 1,426.6 ± 522.23 mm2, whereas the mean surface area for the curved nail was 2,364.6 ± 290.13 mm2. The differences between the two groups were statistically significant (p=0.004). There were 2 straight nail insertions that missed the calcaneus and as such had a significantly lower surface area of bone contact within the calcaneus (557 mm2 and 951 mm2). After completing the measurements, direct visualization of the area reamed in the calcaneus was determined by cross-sectioning each specimen. The curved nail showed more bone-to-nail contact compared with the straight nail (Figure 1).
Tibiotalocalcaneal arthrodesis has become an increasingly popular procedure. The use of intramedullary nailing is beneficial for subtalar and tibiotalar arthritis, posttraumatic injury, as well as a salvage technique for previous failed surgery [1]. One method of achieving this arthrodesis is with the use of an intramedullary nail passed in a retrograde fashion. The intramedullary nail construct has proven to provide biomechanical stiffness in all bending and rotational directions [2]. The majority of intramedullary nails used for tibiocalcaneal arthrodesis are straight in design. However, it has been documented that straight nails often have very little purchase in the calcaneus, often engaging only the sustentaculum tali [3]. This limitation diminishes the calcaneal bone-to-rod interface and thus the stability.
Recent advances in nail design have produced nails with valgus and posterior curves. Previous studies have shown that a nail with a single lateral curve occupies more volume in the calcaneus than a straight nail [4]. However, to our knowledge, there is no report comparing a nail with a distal lateral and posterior bend with the surface area occupied by a straight nail. The purpose of this investigation is to compare the surface area of calcaneal bone contact with a straight nail versus a curved nail with a valgus and posterior bend. MATERIALS & METHODS
Nail Insertion
Seven pairs of embalmed cadaver legs stored at -4°C were thawed at room temperature 12 hours prior to preparation and dissection. The specimens had no visible pathology or deformity and were selected randomly for nail fixation. Each specimen was sectioned at the level of the isthmus to ensure the narrowest of diameters in the tibial shaft. While in contradiction to clinical practice, the joint surfaces were not prepared. This method follows previous cadaveric studies by McGarvey et al. [3] and Pochatko et al. [5]. It is believed that it is easier to hold the correct position of the unprepared specimen and the relationship between the talus and tibia would be unchanged compared to a prepared joint. The foot was then placed in 2-5 degrees of valgus, 90 degrees of foot-to-tibial shaft dorsiflexion, and approximately 10 degrees of external rotation [3]. The position was held in place manually to simulate standard operative techniques. In 1 limb of each pair, a straight nail preparation design was implanted (Orthofix Ankle Compression Nail, Orthofix; Verona, Italy). A 3-mm-diameter Kirschner guide wire was placed in an antegrade fashion through the center of the tibia, through the talus, and into the calcaneus. A rigid 13-mm entry reamer was then used to ream the path for the nail in an antegrade fashion. In the contralateral limb from each pair, a curved nail preparation design was implanted (A3-Anatomic Ankle Arthrodesis System Nail, Small Bone Innovations; Berlin, Germany). This intramedullary nail design includes a distal double bend, 1 posterior and 1 lateral. Adjustments were required for insertion of the curved nail to account for the posterior and lateral curve. First, a 3-mm diameter Kirschner guide wire was placed antegrade through the calcaneus, similar to the straight nail insertion. An offset guide was placed and aligned with the second ray. Using the system-aiming design, a second guide wire was placed through the offset guide in an antegrade fashion to account for the posterolateral curve of the nail. The 13-mm-diameter entry reamer was then passed over the second guide wire in a retrograde fashion across the calcaneus and talus. Reaming was performed by the same person for each paired specimen. The use of a 13-mm reamer was used for both nail designs to account for the 13-mm standard distal diameter of the curved nail design.
Determining Surface Area Bone Contact
After reaming in both paired limbs, soft tissue dissection was performed and the calcaneus was disarticulated from the tibia and talus. The diameters of the entry and exit sites for each calcaneus were recorded and used to calculate the surface area of the cylindrical shape created by reaming. A 3-dimensional digitizer (MicroScribe 3DX, Immersion Corporation; San Jose, CA) and 3-dimensional surface reconstruction software was used to manually digitize the circumference of the entry and exit points reamed in the calcaneus. A 3-dimensional model of the bone in contact with the hindfoot nail was accomplished by triangulating points between entry and exit points in the calcaneus using the digitizer. Surface area was then calculated with a positional accuracy of 0.23 mm. Paired t-tests were used to determine whether the observed differences between the straight and curved nail were significant, with the level of significance set at 0.05. RESULTS The entry and exit diameters for each calcaneus used to calculate the surface area of bone contact are depicted in Table 1. The mean surface area for the straight nail design was 1,426.6 ± 522.23 mm2, whereas the mean surface area for the curved nail was 2,364.6 ± 290.13 mm2. The differences between the two groups were statistically significant (p=0.004). There were 2 straight nail insertions that missed the calcaneus and as such had a significantly lower surface area of bone contact within the calcaneus (557 mm2 and 951 mm2). After completing the measurements, direct visualization of the area reamed in the calcaneus was determined by cross-sectioning each specimen. The curved nail showed more bone-to-nail contact compared with the straight nail (Figure 1).

DISCUSSION
Retrograde intramedullary nailing has increased in popularity with several biomechanical and clinical studies in the literature reporting the effectiveness of intramedullary rods for tibiocalcaneal arthrodesis [1,6-10]. Berend et al. [2] compared stiffness of intramedullary nail fixation versus lagscrew fixation in a cadaveric model and found that the intramedullary nail construct was significantly (p<0.05) stiffer than the crossed lag screw construct in all 4 bending directions and both rotational directions, plantarflexion, dorsiflexion, inversion, eversion, internal rotation, and external rotation. It was surmised that this construct would increase fusion rate through increased stability of the internal fixation. However, an early cadaveric study by McGarvey et al. [3] using an antegrade intramedullary rod insertion to determine the risk of entry site to plantar structures found that the exit site was in the sustentaculum tali and not the calcaneus. This position was thought to reduce the stability of the construct due to minimal bone-to-rod surface area in the calcaneus.
The design of intramedullary nails for tibiotalocalcaneal arthrodesis has evolved to increase the distance from at-risk plantar structures, and to enhance bone coverage of the nail given the anatomical alignment of the bones involved. It is important that the nail has good purchase in the calcaneus and not only in the medial calcaneal wall or sustentaculum tali. Poor calcaneal purchase can lead to calcaneal fracture, loss of fixation, deformity, and lower rate of union [11,12]. It has been shown that the quality of fusion is not only determined by the stiffness of the construct but also by the contact area of the bone surfaces [8,13,14]. In the current study, we used a nail design that contains both a valgus and posterior curve. To our knowledge, there are no previous investigations examining the impact of nail design on this variable.
In this study, our aim was to compare bone contact surface area in the calcaneus between a straight tibiotalocalcaneal nail and a tibiotalocalcaneal nail with a posterior and lateral curve. We found that the tibiotalocalcaneal nail with a posterior and lateral curve had significantly more bone contact surface area than a straight tibiotalocalcaneal nail. The average surface area of bone contact for the curved nail was significantly greater than the straight nail design. One previous report compared the volume of the calcaneus occupied by a straight nail with that of a lateral curved nail. Mückley et al. [4] used computerized tomography to calculate the volume of the intracalcaneal portion of a tibiotalocalcaneal nails. They found that the portion of the nail completely surrounded by bone within the calcaneus did not differ significantly between the 2 devices, a straight nail (3.21 cm3) and 1 with a valgus curve (3.67 cm3). However, the curved nail used in that study only contained a 5 degree valgus curve in the hindfoot area. The advantages of the curved nail design used in the current study are aimed at providing better bone contact within the calcaneus. The lateral bend of the curved nail design respects the physiological hindfoot valgus. Hindfoot valgus results in a laterally shifted position of the calcaneus in relation to the tibia axis. The lateral bend in the nail provides more length inside the calcaneus compared to a straight nail. The additional posterior bend of the nail is designed to account for the posterior shift of the calcaneus in relation to the tibial axis. This posterior bend also allows for more bone contact within the calcaneus while still having an entry point that is located far from tendons and nerves at risk. The distal end of the nail is oblique in relation to the nail axis and parallel to the caudal surface of the calcaneus. This shape allows for the nail to be more in contact with the bone surface of the calcaneus.
There were several limitations of our study. The specimen joint surfaces were not prepared in the usual manner of standard operative technique. However, previous cadaver studies have also excluded preparing the joint surfaces with the reasoning that it does not change the anatomic relationship and the positioning is easier to hold in cadaveric specimens [4,5]. Usually, the guide wires are passed in retrograde fashion using fluoroscopy to verify placement of the wire as well as alignment. However, we did not use fluoroscopy during our study. Instead, we used a method previously described to pass the guide wire in an antegrade fashion [3]. Reaming in an antegrade fashion and using the level of the isthmus would centralize the nail and allow optimal position within the tibial canal [11]. It is likely that the limitations above contributed to 1 of the straight nail specimens not having complete bone contact in the calcaneus. Guide wires inserted down the center of the tibial canal in an antegrade fashion are more likely to enter lateral to the midline of the talus and miss the medial portion of the body of the calcaneus. McGarvey et al. [3] showed that all specimens involved in the first portion of their study revealed an exit point in the sustentaculum tali or at the junction of the sustectaculum and medial calcaneal wall. The second portion of their study showed better bone contact but required medialization of the hindfoot and resection of the medial malleolus. Use of a curved nail eliminates the potential of the nail not having adequate bone contact and the need to medialize the talus.
The goals of tibiotalocalcaneal arthrodesis are to provide stable fixation, correct hindfoot alignment, and achieve good contact between bone surfaces to obtain union. A nail design that can improve compression and bone contact will likely lead to higher fusion rates and stability. The results of this cadaveric study demonstrated that tibiotalocalcaneal nails with a posterior and lateral curve provide significantly more bone contact surface area. REFERENCES [1] Chou LB, Mann RA, Yaszay B, Graves SC, McPeake WT, Dreeben SM, Horton GA, Katcherian DA, Clanton TO, Miller RA, Van Manen JW. Tibiotalocalcaneal arthrodesis. Foot Ankle Int. 2000;21(10):804-8.
[2] Berend ME, Glisson RR, Nunley JA. A biomechanical comparison of intramedullary nail and crossed lag screw fixation for tibio- talocalcaneal arthrodesis. Foot Ankle Int. 1997;18(10):639-43.
[3] McGarvey WC, Trevino SG, Baxter DE, Noble PC, Schon LC. Tibiotalocalcaneal arthrodesis: anatomic and technical considerations. Foot Ankle Int. 1998;19(6):363-9.
[4] Mückley T, Ullm S, Petrovitch A, Klos K, Beimel C, Fröber R, Hofmann GO. Comparison of two intramedullary nails for tibiocalcaneal fusion: anatomic and radiographic considerations. Foot Ankle Int. 2007;28(5):605-12.
[5] Pochatko DJ, Smith JW, Phillips RA, Prince BD, Hedrick MR. Anatomic structures at risk: combined subtalar and ankle arthrodesis with a retrograde intramedullary rod. Foot Ankle Int. 1995;16(9):542-7.
[6] Hammett R, Hepple S, Forster B, Winson I. Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail. The results of 52 procedures. Foot Ankle Int. 2005;26(10):810-15.
[7] Millett PJ, O’Malley MJ, Tolo ET, Gallina J, Fealy S, Helfet DL. Tibiotalocalcaneal fusion with a retrograde intramedullary nail: clinical and functional outcomes. Am J Orthop. 2002;31(9):531-6.
[8] Mückley T, Eichhorn S, Hoffmeier K, von Oldenburg G, Speitling A, Hoffmann GO, Bühren V. Biomechanical evaluation of primary stiffness of tibiotalocalcaneal fusion with intramedullary nails. Foot Ankle Int. 2007;28(2):224-31.
[9] Mückley T, Klos K, Dreschel T, Beimel C, Gras F, Hofmann GO. Short-term outcome of retrograde tibiocalcaneal arthrodesis with a curved intramedullary nail. Foot Ankle Int. 2011;32(1):47-56.
[10] Rammelt S, Pyrc J, Agren P, Hartsock LA, Cronier P, Friscia DA, Hansen ST, Schaser K, Ljungqvist J, Sands AK. Tibiocalcaneal fusion using hindfoot arthrodesis nail: a multicenter study. Foot Ankle Int. 2013;34(9):1245-55.
[11] Hyer CF, Cheney N. Anatomic aspects of tibiocalcaneal nail arthrodesis. J Foot Ankle Surg. 2013;52(6):724-7.
[12] Thomas RL, Sathe V, Habib SI. The use of intramedullary nails in tibiocalcaneal arthrodesis. J Am Acad Orthop Surg. 2012;20(1):1-7.
[13] Hintermann B, Valderrabano V, Nigg B. Influence of Screw type on obtained contact area and contact force in a cadaveric subtalar arthrodesis model. Foot Ankle Int. 2002;23(11):986-91.
[14] Wilson FC, Fay GF, Lamotte P. Triple arthrodesis: a study of the factors affecting fusion after 301 procedures. J Bone Joint Surg Am. 1965;47A:340-8.
There were several limitations of our study. The specimen joint surfaces were not prepared in the usual manner of standard operative technique. However, previous cadaver studies have also excluded preparing the joint surfaces with the reasoning that it does not change the anatomic relationship and the positioning is easier to hold in cadaveric specimens [4,5]. Usually, the guide wires are passed in retrograde fashion using fluoroscopy to verify placement of the wire as well as alignment. However, we did not use fluoroscopy during our study. Instead, we used a method previously described to pass the guide wire in an antegrade fashion [3]. Reaming in an antegrade fashion and using the level of the isthmus would centralize the nail and allow optimal position within the tibial canal [11]. It is likely that the limitations above contributed to 1 of the straight nail specimens not having complete bone contact in the calcaneus. Guide wires inserted down the center of the tibial canal in an antegrade fashion are more likely to enter lateral to the midline of the talus and miss the medial portion of the body of the calcaneus. McGarvey et al. [3] showed that all specimens involved in the first portion of their study revealed an exit point in the sustentaculum tali or at the junction of the sustectaculum and medial calcaneal wall. The second portion of their study showed better bone contact but required medialization of the hindfoot and resection of the medial malleolus. Use of a curved nail eliminates the potential of the nail not having adequate bone contact and the need to medialize the talus.
The goals of tibiotalocalcaneal arthrodesis are to provide stable fixation, correct hindfoot alignment, and achieve good contact between bone surfaces to obtain union. A nail design that can improve compression and bone contact will likely lead to higher fusion rates and stability. The results of this cadaveric study demonstrated that tibiotalocalcaneal nails with a posterior and lateral curve provide significantly more bone contact surface area. REFERENCES [1] Chou LB, Mann RA, Yaszay B, Graves SC, McPeake WT, Dreeben SM, Horton GA, Katcherian DA, Clanton TO, Miller RA, Van Manen JW. Tibiotalocalcaneal arthrodesis. Foot Ankle Int. 2000;21(10):804-8.
[2] Berend ME, Glisson RR, Nunley JA. A biomechanical comparison of intramedullary nail and crossed lag screw fixation for tibio- talocalcaneal arthrodesis. Foot Ankle Int. 1997;18(10):639-43.
[3] McGarvey WC, Trevino SG, Baxter DE, Noble PC, Schon LC. Tibiotalocalcaneal arthrodesis: anatomic and technical considerations. Foot Ankle Int. 1998;19(6):363-9.
[4] Mückley T, Ullm S, Petrovitch A, Klos K, Beimel C, Fröber R, Hofmann GO. Comparison of two intramedullary nails for tibiocalcaneal fusion: anatomic and radiographic considerations. Foot Ankle Int. 2007;28(5):605-12.
[5] Pochatko DJ, Smith JW, Phillips RA, Prince BD, Hedrick MR. Anatomic structures at risk: combined subtalar and ankle arthrodesis with a retrograde intramedullary rod. Foot Ankle Int. 1995;16(9):542-7.
[6] Hammett R, Hepple S, Forster B, Winson I. Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail. The results of 52 procedures. Foot Ankle Int. 2005;26(10):810-15.
[7] Millett PJ, O’Malley MJ, Tolo ET, Gallina J, Fealy S, Helfet DL. Tibiotalocalcaneal fusion with a retrograde intramedullary nail: clinical and functional outcomes. Am J Orthop. 2002;31(9):531-6.
[8] Mückley T, Eichhorn S, Hoffmeier K, von Oldenburg G, Speitling A, Hoffmann GO, Bühren V. Biomechanical evaluation of primary stiffness of tibiotalocalcaneal fusion with intramedullary nails. Foot Ankle Int. 2007;28(2):224-31.
[9] Mückley T, Klos K, Dreschel T, Beimel C, Gras F, Hofmann GO. Short-term outcome of retrograde tibiocalcaneal arthrodesis with a curved intramedullary nail. Foot Ankle Int. 2011;32(1):47-56.
[10] Rammelt S, Pyrc J, Agren P, Hartsock LA, Cronier P, Friscia DA, Hansen ST, Schaser K, Ljungqvist J, Sands AK. Tibiocalcaneal fusion using hindfoot arthrodesis nail: a multicenter study. Foot Ankle Int. 2013;34(9):1245-55.
[11] Hyer CF, Cheney N. Anatomic aspects of tibiocalcaneal nail arthrodesis. J Foot Ankle Surg. 2013;52(6):724-7.
[12] Thomas RL, Sathe V, Habib SI. The use of intramedullary nails in tibiocalcaneal arthrodesis. J Am Acad Orthop Surg. 2012;20(1):1-7.
[13] Hintermann B, Valderrabano V, Nigg B. Influence of Screw type on obtained contact area and contact force in a cadaveric subtalar arthrodesis model. Foot Ankle Int. 2002;23(11):986-91.
[14] Wilson FC, Fay GF, Lamotte P. Triple arthrodesis: a study of the factors affecting fusion after 301 procedures. J Bone Joint Surg Am. 1965;47A:340-8.